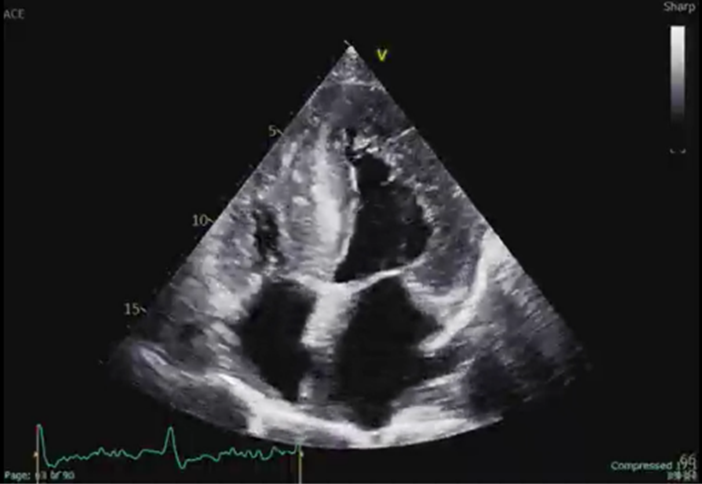
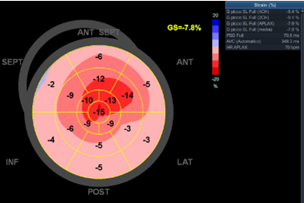
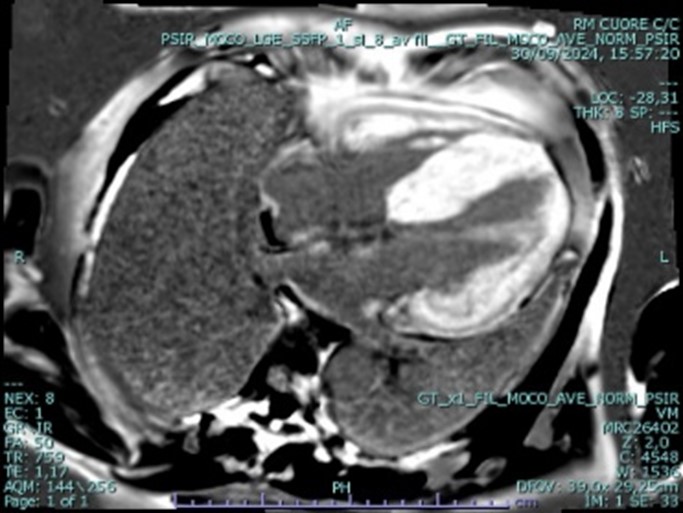
Background: Cardiac amyloidosis (CA) is a progressive infiltrative cardiomyopathy commonly linked to heart failure (HF) symptoms. Ventricular arrhythmias (VA) may occur in a small subset of patients, typically in advanced stages when amyloid deposits compromise myocardial and conduction system integrity. Managing VA in asymptomatic patients with CA remains complex and debated, particularly regarding beta-blockers due to potential adverse effects. Clinical case: A 65-year-old male, an experienced runner (10 km/day), presented for a primary prevention cardiological assessment. His history included dyslipidemia and smoking. He denied symptoms such as dyspnea, angina, syncope or palpitations. An electrocardiogram (ECG) showed sinus bradycardia, first-degree AV block, inferoseptal QS waves and altered lateral leads repolarization. Recent transthoracic echocardiography (TTE) suggested hypertrophic cardiomyopathy. 24-hour ECG Holter monitoring identified frequent asymptomatic non-sustained ventricular tachycardia (NSVT), prompting Emergency Department evaluation. Blood tests showed normal complete blood count, electrolytes, and thyroid function, with Troponin T at 55 ng/L, CK-MB 7.5 ng/mL, BNP 219 pg/mL, and NT-proBNP 3776 pg/mL. During hospitalization in our Cardiology department, the patient remained asymptomatic. Complete TTE showed severe biventricular wall thickening with a granular sparkling appearance, severe impairment of global left ventricular (LV) longitudinal myocardial deformation (GLS = -7.8%) with “apical sparing” pattern, a mildly impaired LV ejection fraction (EF), LV diastolic dysfunction, and thickening of interatrial septum, raising suspicion for cardiac amyloidosis. Tests for AL amyloidosis were negative, including serum/urine immunofixation and free light chain assay (kappa/lambda). Bone scintigraphy (99mTc-HMDP) revealed a Perugini score of 3. Cardiac magnetic resonance imaging confirmed severe increase in LV wall thickness with global hypokinesia (LVEF of 41%) and extensive biventricular late gadolinium enhancement, sparing the apical segments. Coronary angiography found no significant lesions. Telemetry documented recurrent asymptomatic NSVT episodes, leading to initiation of bisoprolol, titrated to 2.5 mg twice daily. The patient was discharged on this well-tolerated regimen, which reduced the arrhythmic burden. HF therapy was initiated. Genetic testing for transthyretin CA and extended genetic analysis for cardiomyopathies are ongoing.