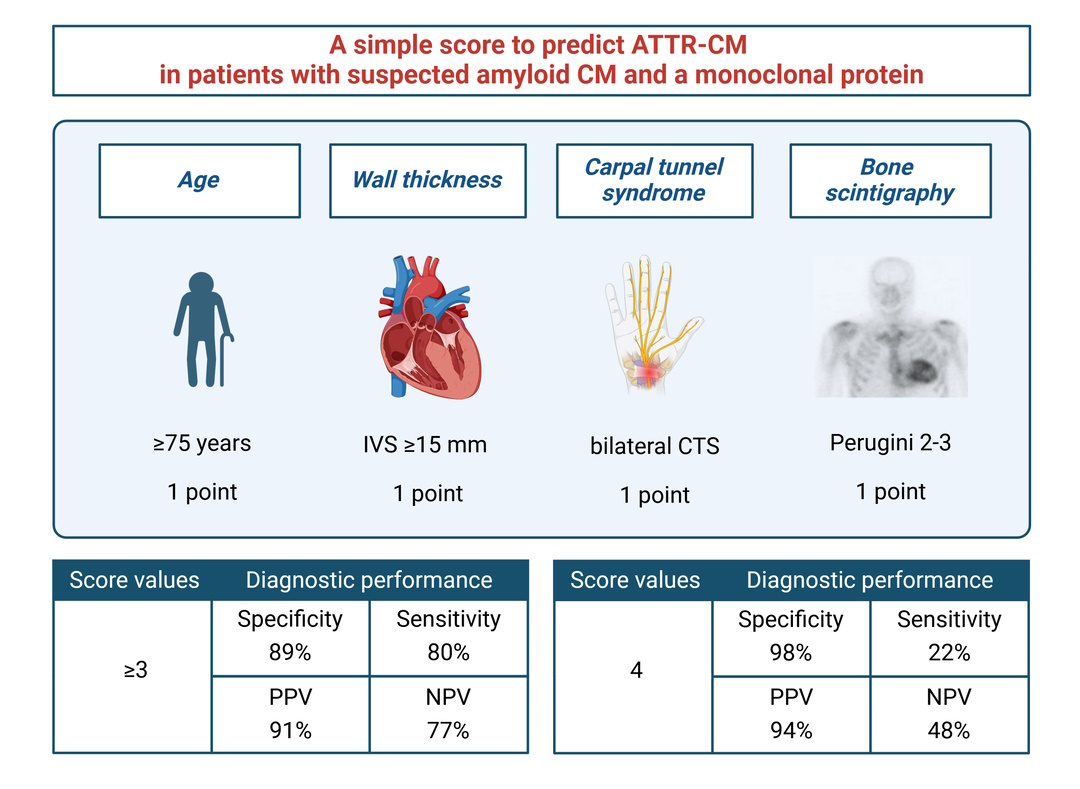
Background: Amyloid cardiomyopathy (CM) is increasingly recognized as an important cause of heart failure. In patients with suspected amyloid CM, the presence of a monoclonal protein may indicate light-chain (AL) amyloidosis or may be an incidental finding in those with transthyretin (ATTR) amyloidosis. AL- and ATTR-CM require different treatments, and untreated AL-CM progresses much more rapidly than untreated ATTR-CM. Distinguishing between AL-CM and ATTR-CM can help determine both the timing and site of tissue biopsy, especially given the low sensitivity of peripheral biopsies. Methods: We retrieved data of 141 patients evaluated in 8 referral centers for suspected amyloid CM since May 2021 to December 2024, undergoing tissue biopsy because of a monoclonal protein and/or Perugini grade 1. These patients had no history of hematological disorder, possibly except for monoclonal gammopathy of unknown significance (MGUS). Results: Only 6 patients (4%) underwent tissue biopsy because of a Perugini grade 1. Among the remaining 135 patients, who had a monoclonal protein, 105 (78%) underwent a peripheral tissue biopsy, but 74 (55%) still required an endomyocardial biopsy. The majority of the 135 patients had ATTR-CM (n=76, 56%), followed by AL-CM (n=55, 41%). The most prominent differences between patients with ATTR- vs. AL-CM were an older age, a greater interventricular septal (IVS) thickness at echo, no vs. mono- vs. bilateral carpal tunnel syndrome, and Perugini grade 2-3 (all p<0.001). We created a simple score including age ≥75 years, IVS thickness ≥15 mm, bilateral CTS, and Perugini grade 2-3, with 1 point for each element. Score values 3 or 4 had a 80% sensitivity, 89% specificity, 91% positive predictive value, and 77% negative predictive value for ATTR-CM. A score value of 4 had a 98% specificity and 94% positive predictive value for ATTR-CM. Conclusions: In patients with suspected amyloid CM and a monoclonal protein, the following variables may be considered: age ≥75 years, IVS thickness ≥15 mm, bilateral CTS, and Perugini grade 2-3. If at least 3 of these features are present, the specificity for the final diagnosis of ATTR-CM approaches 90%, and is almost 100% when all four of them are present. In other words, patients with these features are much more likely to have ATTR- instead of AL-CM, although histological confirmation is still required to reach a definite diagnosis.