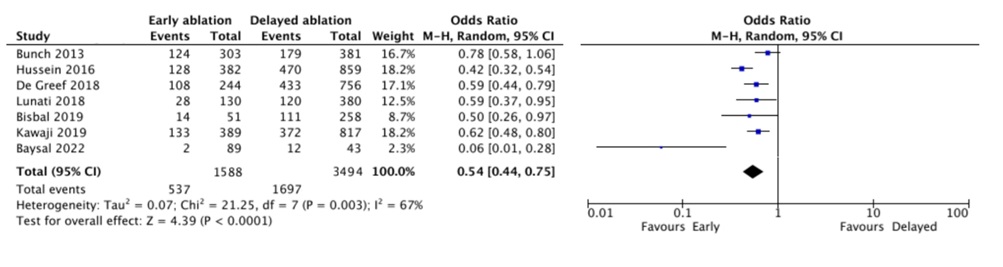
Background: The optimal timing for catheter ablation (CA) in patients with atrial fibrillation (AF) remains uncertain. Objective: This study aims to evaluate whether early catheter ablation (within 1 year of diagnosis) compared to delayed catheter ablation (≥1 year) is associated with a lower rate of arrhythmia recurrence. Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we searched Medline, Embase, and Scopus to identify all observational studies published up to October 2024 that compared the risk of AF recurrence in patients treated with early or delayed CA. The risk of AF recurrence was assessed using the Mantel-Haenszel random effects model, with odds ratios as the effect measure and 95% confidence intervals (CIs). Heterogeneity was evaluated using the Higgins I² statistic, while multivariable meta-regression analysis was conducted to analyse sources of heterogeneity. Results: Seven studies involving 5,082 patients with AF (mean age 60.2 ± 5.9 years) were included in the final analysis. Among these, 1,588 patients (31.2%) underwent early CA, defined as within one year of AF diagnosis. The pooled analysis using a random effects model indicated that early CA was associated with a significantly lower risk of AF recurrence (OR: 0.54; 95% CI: 0.44 to 0.75; I²: 42%) after a mean follow-up of 3.4 ± 0.4 years. Multivariate regression analysis revealed that the risk of AF recurrence was significantly influenced by age (p = 0.001), male sex (p = 0.02), body mass index (p = 0.003), and length of AF history (p < 0.001). Conclusion: Early CA in patients with atrial fibrillation is associated with a significantly lower risk of arrhythmia recurrence compared to delayed ablation.