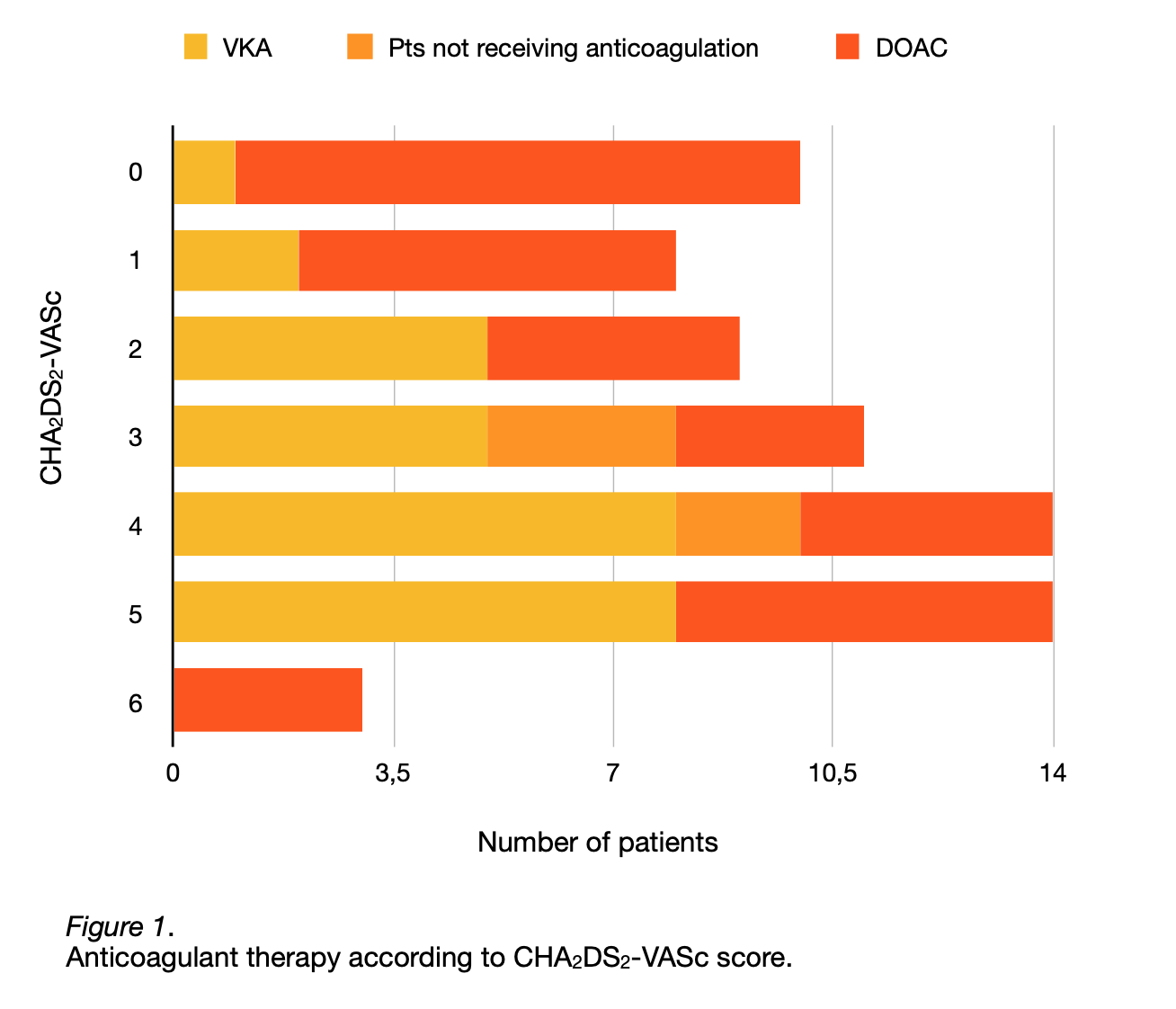
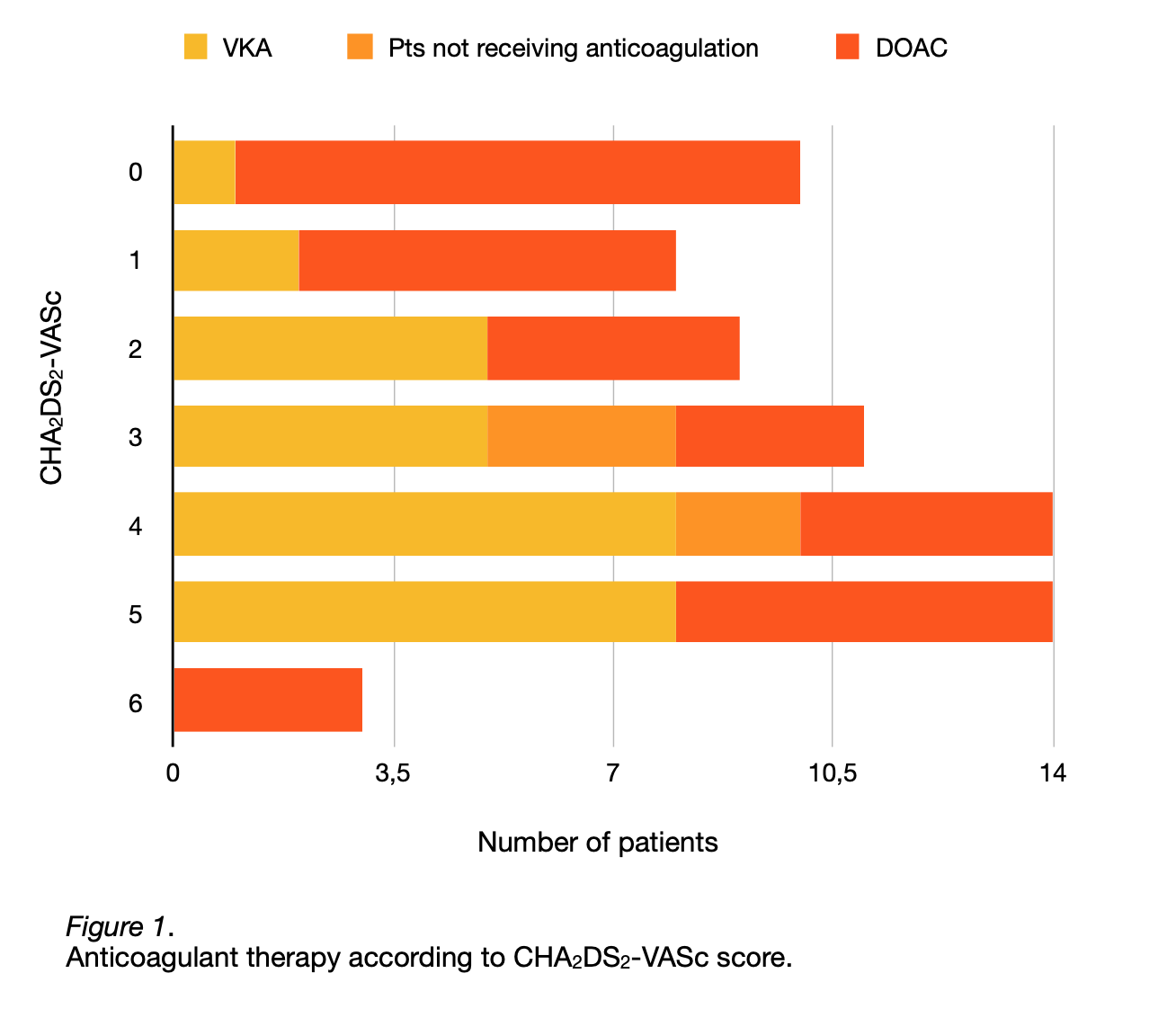
Rationale and aim Based on latest European guidelines, all patients with hypertrophic cardiomyopathy (HCM) and atrial fibrillation (AF) should receive anticoagulant therapy irrespective of their thrombotic risk measured by CHA2DS2-VA score (CHA2DS2-VASc score before 2024 guidelines). The aim of our study was to assess the implementation and type of anticoagulant therapy prescribed in patients with HCM in real-world practice. Methods We retrospectively included 69 patients with a diagnosis of both AF and HCM admitted to our Cardiology ward during the last 9 years. We then classified each patient according to their CHA2DS2-VASc score into seven arms (score 0 to 6). Subsequently, in each arm we evaluated the amount of patients prescribed with anticoagulant therapy, either direct oral anticoagulant (DOAC) or vitamin-K antagonist (VKA), versus patients not treated with anticoagulant. Results Our results show that anticoagulant therapy is prescribed in the vast majority of patients (92.8%). The minority of subjects not receiving anticoagulant (7.2%) has a CHA2DS2-VASc score of 3 or 4 whereas in the other arms no patient is represented (Figure 1). When anticoagulation is prescribed, DOACs are preferred over VKAs in patients with CHA2DS2-VASc score either low or very high while in subjects with CHA2DS2-VASc score of 2 to 5 VKA represents the most commonly prescribed therapy. In the highest CHA2DS2-VASc score arm, DOACs seem to be the only therapeutic option. Conclusions This study demonstrates that our clinical practice in prescribing anticoagulant therapy is not far from recent guidelines recommendations. The high rate of subjects receiving anticoagulant shows that only a small percentage of patients is exposed to increased embolic risk related to AF due to increased hemorrhagic risk or to absolute contraindications to anticoagulant therapy. Such high-risk patients have CHA2DS2-VASc score of 3 or 4 confirming previous data showing that the higher the thromboembolic risk the greater the bleeding risk. In this particular setting all attempts should be done to minimise bleeding risk thus allowing safe implementation of anticoagulant therapy. Compared to non-HCM patients with AF, VKA is overrepresented and this can be partly explained by the initial lack of prospective data about DOACs in HCM.