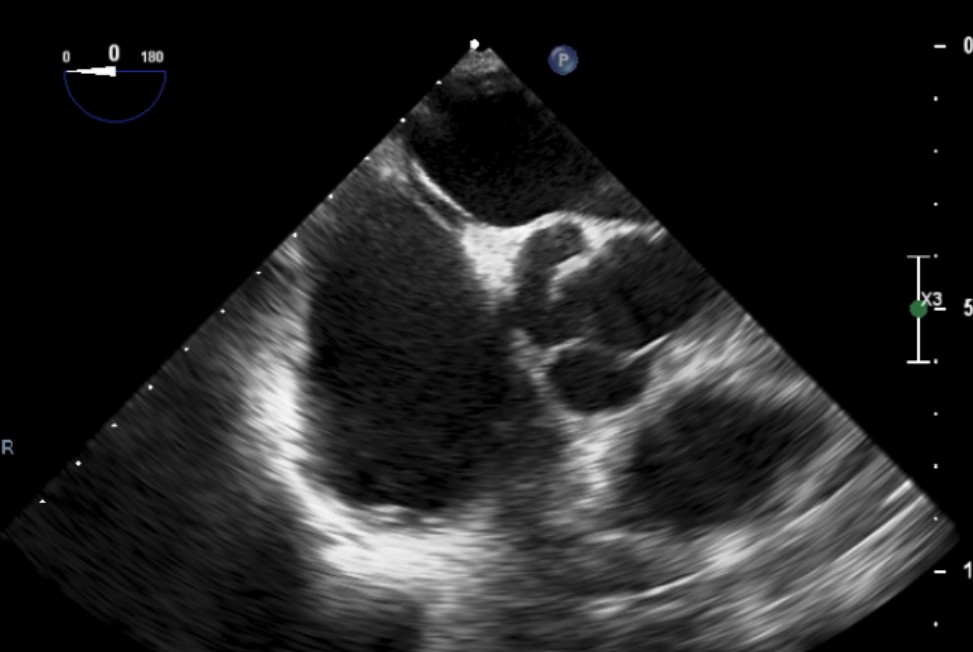
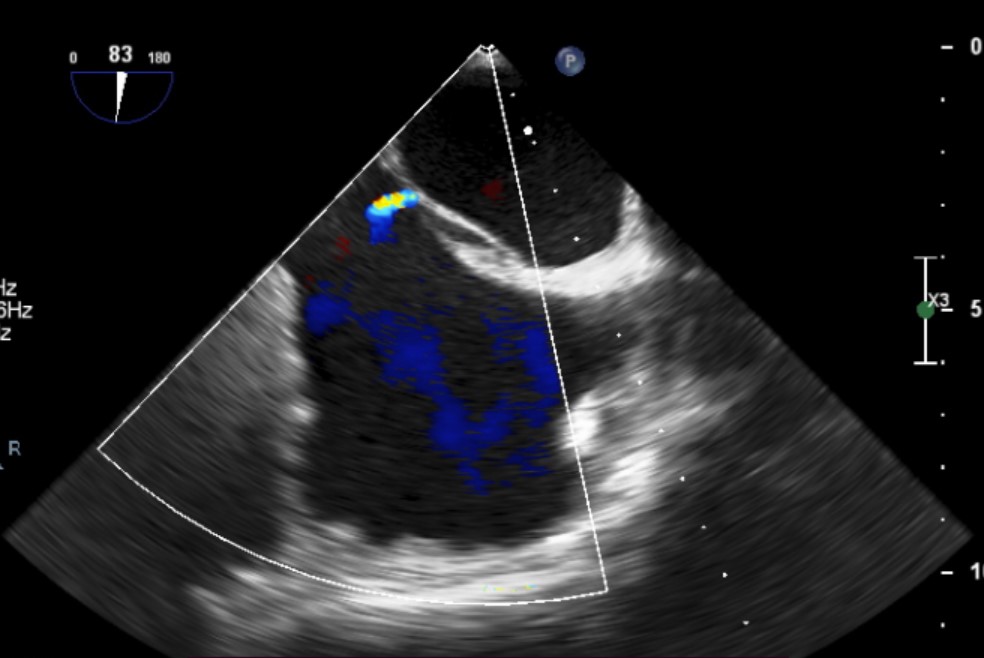
Introduction Double atrial septum (DIAS) is a very rare congenital abnormality, mostly asymptomatic, in which two septa separate the atria, with a chamber between the two septa (IAC). In rare cases, it may predispose to thromboembolic events (STROKE or TIA), which can occur due to blood stasis in the space between the two septa. Case Report A 62-year old Albanian man, diabetic, and smoker was admitted to our ward for atrial fibrillation cardioversion (CVE). He was anticoagulated with Edoxaban 60 mg. Coronary angiography was negative for coronary artery disease. Before CVE, transesophageal echocardiogram showed no thrombi and normal left atrial appendage emptying velocity (47 cm/sec). The examination revealed a double membrane structure (two septa) enclosing an IAC (dimensions 2 x 0.5 mm). IAC separated the septum primum from an accessory atrial septum (AAS). No thrombotic formations were in IAC, while a small ostium secundum-like interatrial defect (maximum size 1.8 mm) was at the inferoposterior part of the small interatrial cavity and showed mild left-to-right shunt. Indeed, CVE did not restore sinus rhythm, thus ablation was recommended. Discussion DIAS is a very rare case. The presence of a distinct AAS at the right of the septum primum and enclosing an IAC below the level of the upper limbus distinguishes our case from a deviation of the atrial septum primum. It could result from the incomplete fusion of the primum and secundum septa and persistence of the left venous valve of the venous sinus. Most of cases were observed in children and were often associated with left heart abnormalities, as the AAS caused obstruction to the blood flow from the right atrium to the left atrium during gestation. Generally, no other concurrent abnormalities are in these patients. Indeed, they are predisposed to thromboembolic events due to blood stasis within the IAC. Shunt direction is crucial for estimating thromboembolic risk, but need for anticoagulation is not definitely recommended. Our patient showed left-to-right shunt which do not involved IAC, thus considering him at lower thromboembolic risk. The literature also considered interatrial defects as challenging when considering procedures that require transseptal punctures such as ablation. Conclusion: DIAS is associated to thromboembolic risk but anticoagulation issues still remains for the treatments of these patients. Further researches are needed in order to optimize therapies in DIAS.