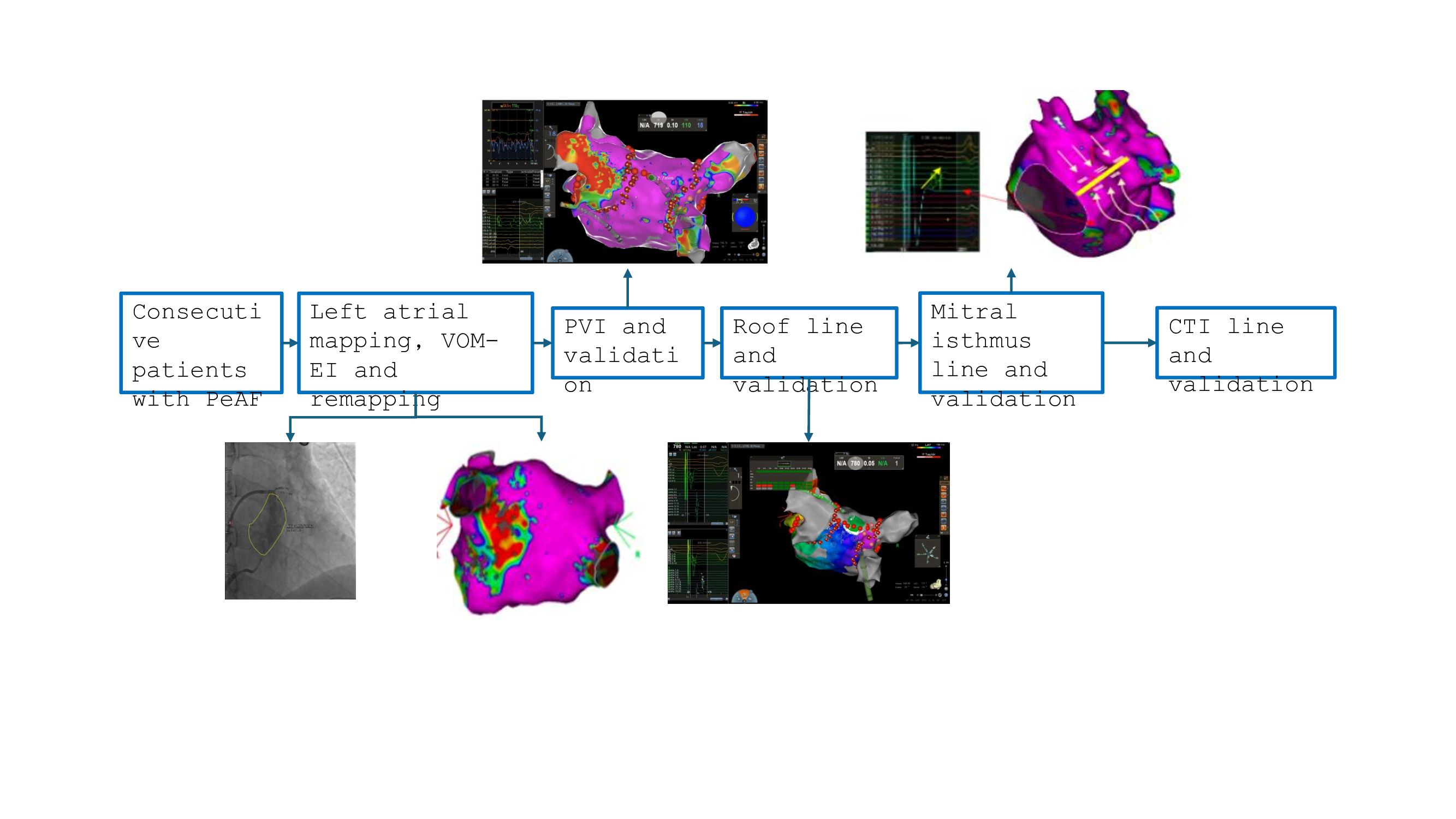
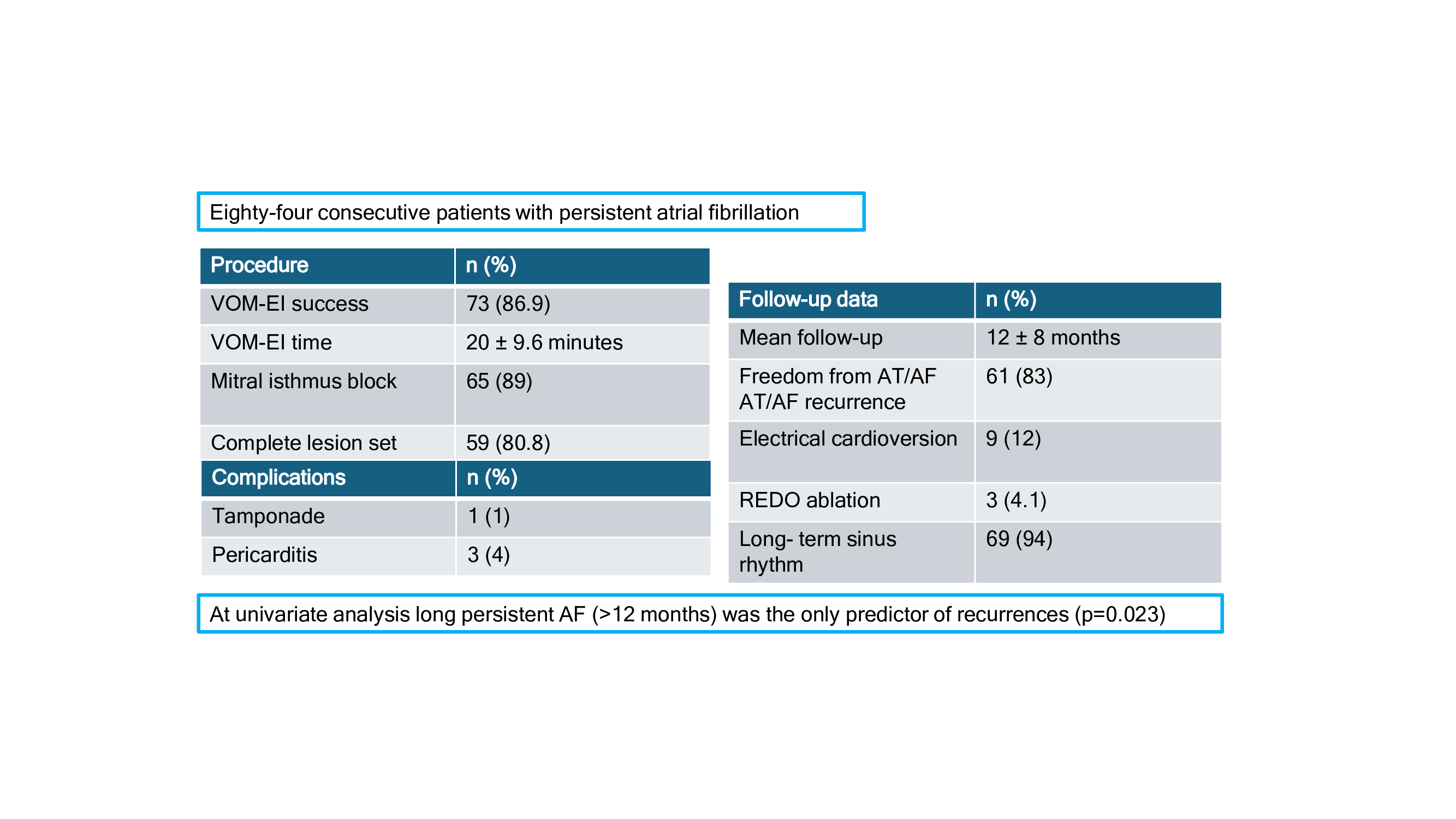
Background: The optimal ablation treatment for persistent atrial fibrillation (PeAF) patients is still debated. The vein of Marshall ethanol infusion (VOM-EI) seems to be a good option but more data need. Purpose: The aim of our study is to evaluate the incidence of AF recurrences in a PeAF population treated with a standard ablation approach consisting of VOM-EI combined with a linear set of ablation lesions. Methods: Consecutive patients undergoing the first ablation procedure of catheter ablation (CA) for PeAF were enrolled. All patients underwent VOM-EI, pulmonary vein isolation, a left atrial (LA) roofline (validated by pacing), mitral line (guided by the newly formed lesion after alcohol infusion into the VOM and validated by pacing from LA appendage) and cavotricuspid isthmus line. LA voltage mapping before and after VOM-EI was also performed. Results: Eighty-four consecutive patients affected by PeAF were included in this study. In 8 patients (9%) VOM-EI was not performed because of the absence of VOM. Seventy-three patients (65 ± 8 years and 78% male) underwent VOM-EI. PV isolation and lines were validated in all subjects. The VOM-EI procedural time is 20 ± 9.6 min. The ML block was achieved in 65 (89%) patients in a mean time of within 7.3 ± 6.9 min. One (1%) cardiac tamponade and three (4%) pericarditis occurred. At a mean follow-up of 12 ± 8 months, 61 out of 73 (83%) patients remained free from AT/AF recurrences after a blanking period of 2 months. Nine patients (12%) needs electrical cardioversion. Three patients (4.1%) underwent REDO ablation. At the end follow-up 69 (94%) patients maintained sinus rhythm. At univariate analysis long persistent AF (>12 months) was the only predictor of recurrences (p=0.023). Conclusions: In our experience VOM-EI systematically combined with an anatomical ablation set was safe and effective in maintaining sinus rhythm in patients with PeAF, in particular in patients with AF < 12 months.