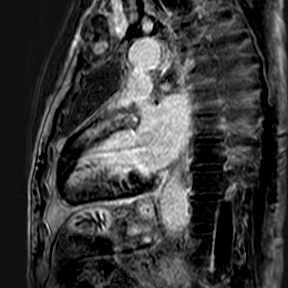
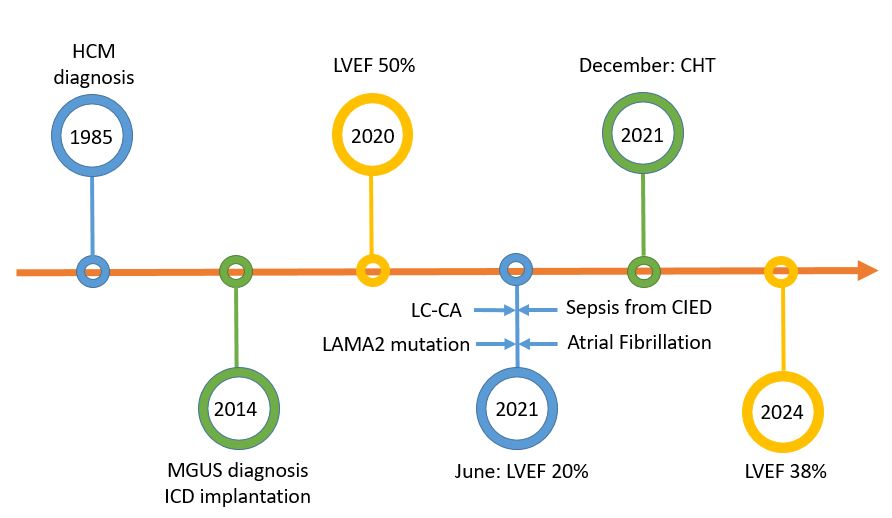
Background: Immunoglobulin light chain amyloidosis (LC-A) is a clonal, nonproliferative plasma cell disorder in which fragments of immunoglobulin light or heavy chain are deposited in tissues. The major determinant of outcome in LC-A is the extent of cardiac involvement. Both hypertrophic cardiomyopathy (HCM) and cardiac amyloidosis (CA) present with increased myocardial thickness and mass. The delayed enhancement patterns on cardiac magnetic resonance imaging (CMR) are thought to distinguish these two diseases. Clinical case: We describe the case of a 61-year-old male patient with a history of non-obstructive HCM since the age of 25 and Monoclonal Gammopathy of Undetermined Significance (MGUS) IgG/IgM lambda. He had a dual-chamber Implantable Cardioverter Defibrillator (ICD) for primary prevention (arrhythmic risk). In 2020 he had an ejection fraction (EF) at the lower limit of normal (50%). In 2021 he was admitted to the cardiology department for atrial fibrillation complicated by left atrial thrombus with cerebral and splanchnic embolization; he had septic shock caused by cardiac implantable electronic device-related infective endocarditis (CIED-IE) originating from urinary tract infection. An hypokinetic-dilated left ventricular cardiomyopathy was observed (EF 20%). Genetic testing was performed, revealing a pathogenic mutation in MYBPC3 (myosin binding protein C) and LAMA2 (laminin-α2 deficiency). A CMR documented an infiltrative cardiomyopathy. A biopsy of the peri-umbilical fat revealed amyloid deposition, positive for immunoglobulin light chains. An osteomedullary biopsy showed a plasma cell infiltrate (9%) and no amyloid substance. A total body scintigraphy with bone tracer showed Perugini score 0. The final diagnosis was LC-A with renal and cardiac involvement. The patient was treated for CIED-IE with antibiotic therapy and removal of the catheters and for LC-CA with five cycles of chemotherapy resulting in complete hematologic response and partial recovery of EF (38%). Conclusions: LC-A is a condition with a poor prognosis, leading to end-stage organ dysfunction. In this patient, the history of HCM likely resulted in a delayed diagnosis due to the overlap of hypertrophic phenotypes. CMR proves to be an excellent tool in the differential diagnosis of hypertrophic phenotypes and should always be performed in the follow-up of HCM, particularly in the presence of clinical changes and left ventricular function variations.