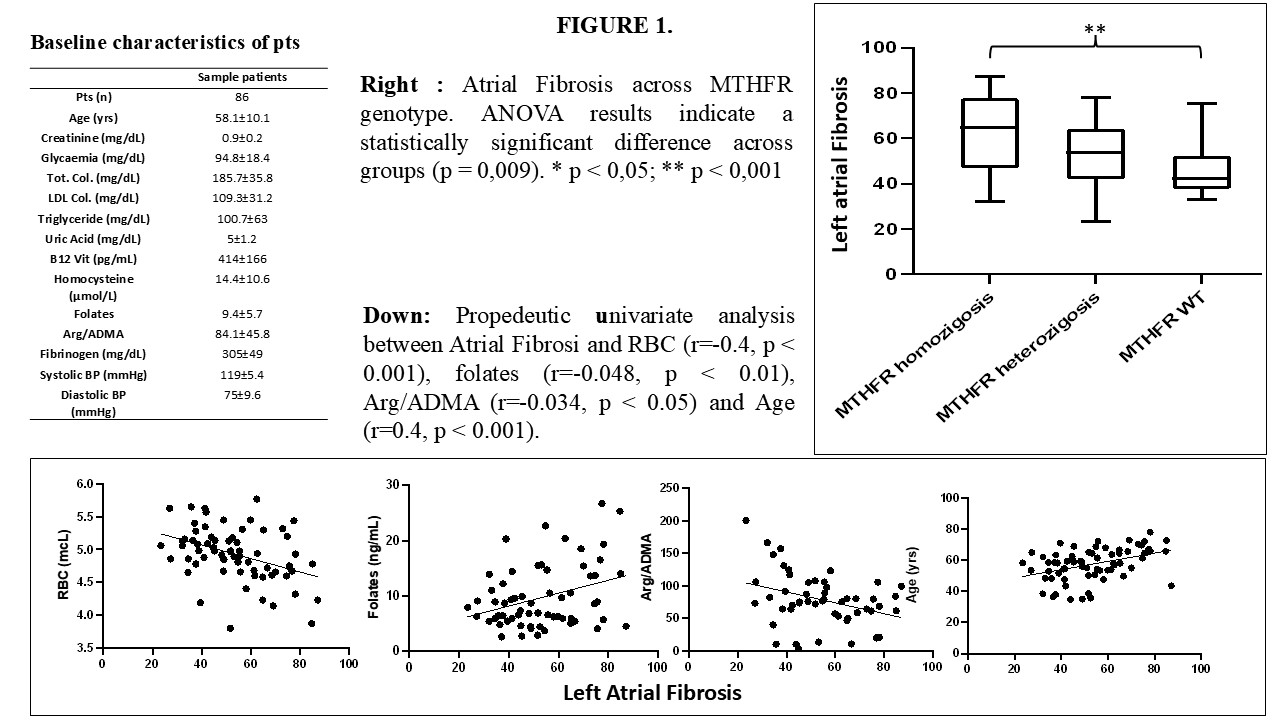
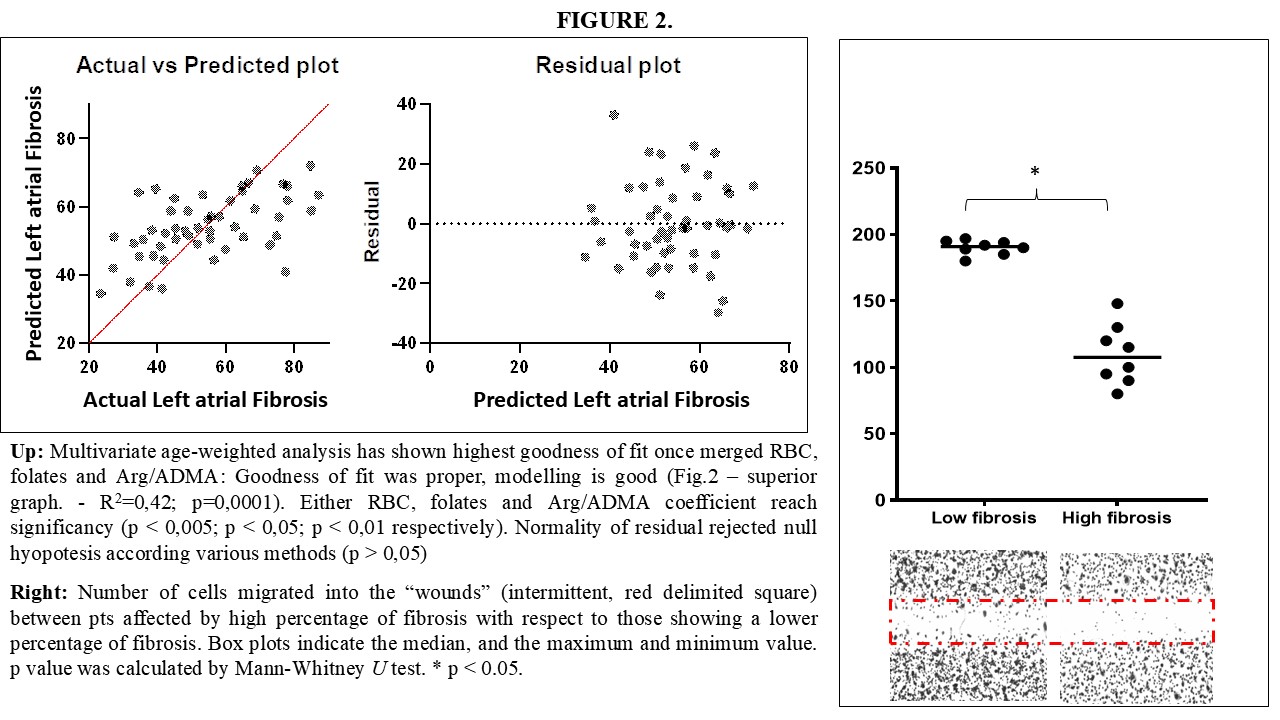
Background: It is accepted that Atrial Fibrillation (AF) does not explain the wholeness of embolic strokes, this forcing postulation of a broader Atrial Cardiomyopathy (AC) entity. Left atrial fibrosis (Fib) is the marker of AC but its pathogenesis is not focused. Folate cycle disorders (FCD) are a dysmetabolism partly explained by MTHFR-inherited defects, leading to stroke. FCD can hinder both methyl handling, thus causing endothelial dysfunction (ED) via Arg/ADMA decrease, and circulating endothelial progenitor cell (EPCs) functioning. Focusing relationship between Fib and FCD might unravel AC pathogenesis. Purpose: We aim to enquire for the hypothesis that: Fib relates to: 1) FCD surrogates, explored through a)Sieric folates, b)MTHFR mutations and c)Arg/ADMA. 2) Dysfunctional EPCs enquired through wound healing assay (WHA). Methods: We studied 86 consecutive patients admitted to the Cardiology Unit of the General Hospital "F.Miulli", subjected to paroxysmal AF ablation. Fib was quantified by relative % of low-voltage (<0,5 mV) bipolar peak-to-peak points. Blood count cell was evaluated. MTHFR C677T genotypes elucidated. Folate were measured by a commercial test. EPCs were isolated (CD45-, CD34+, CD133+, VEGFR2+) and cultured to be subjected to WHA. Results: Univariate analysis seeked for predictive variables (Fig1. bottom graphs). MTHFR ANOVA analysis across Fib was statistically significant (Fig. 1 – right graph. p < 0.01), nonetheless, MTHFR logistic regression did not pass multivariate analysis. A stepwise forward analysis was performed. Since aging is a non modifiable risk factor, a multivariate age-weighted least square regression analysis was performed. The model shows a R-squared of 0.417, indicating a moderately strong correlation between independent variables (RBC, Folates, Arg/ADMA) and dependent variable (Fib)-(Fig.2 – superior graph. – p < 0,0001). Every 1-unit increase in RBC, Arg/ADMA and folates, Fib respectively decreases by 18.5% for RBC, 0,1% for Arg/ADMA and increases by 0,9% for folates. WHA showed a significantly reduced reparative potential of high-Fib derived EPCs with respect to low-Fib. Conclusions: Our findings support the hypothesis that, apart from aging, FCD causing folate-resistence, intended as an higher folic sieric status, relies to a greater extent of Fib in the context of AC and such pathogenic mechanism arise from bone-marrow since both red-hypoglobulinemia and EPCs dysfunction are over-expressed in high Fib.