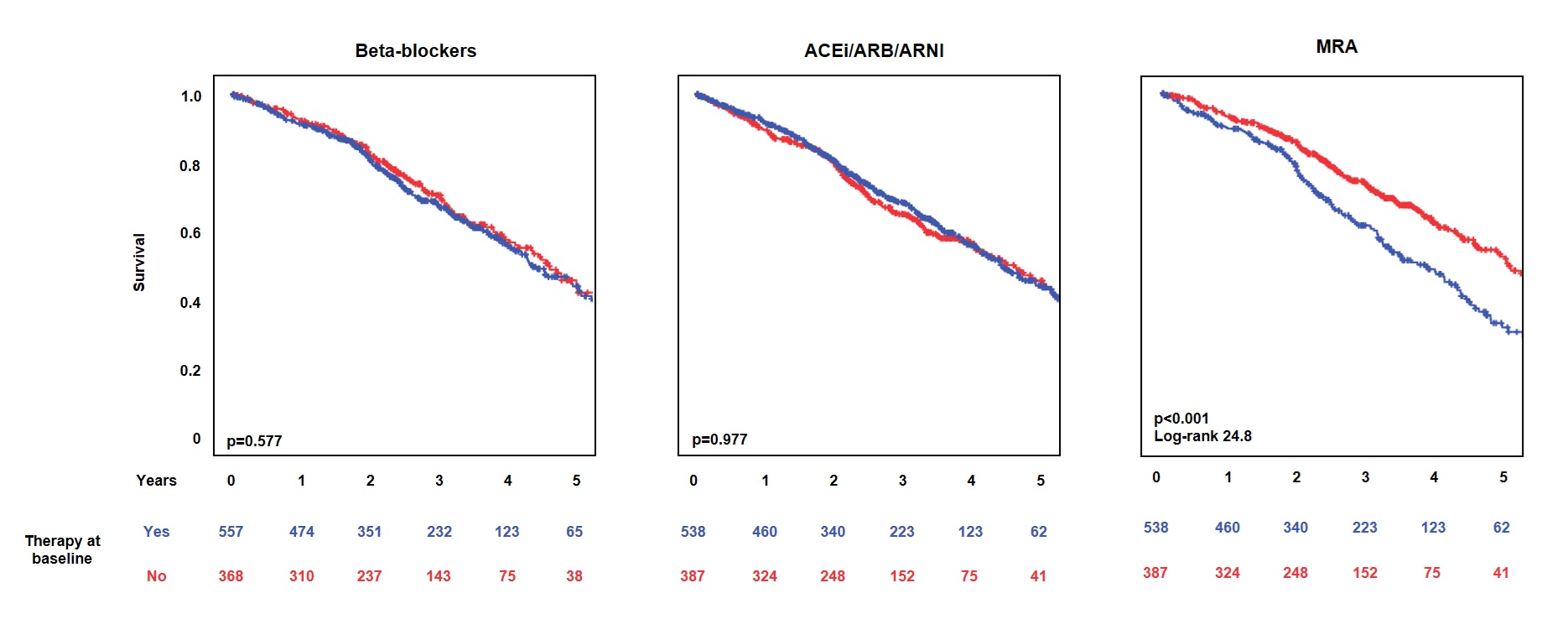
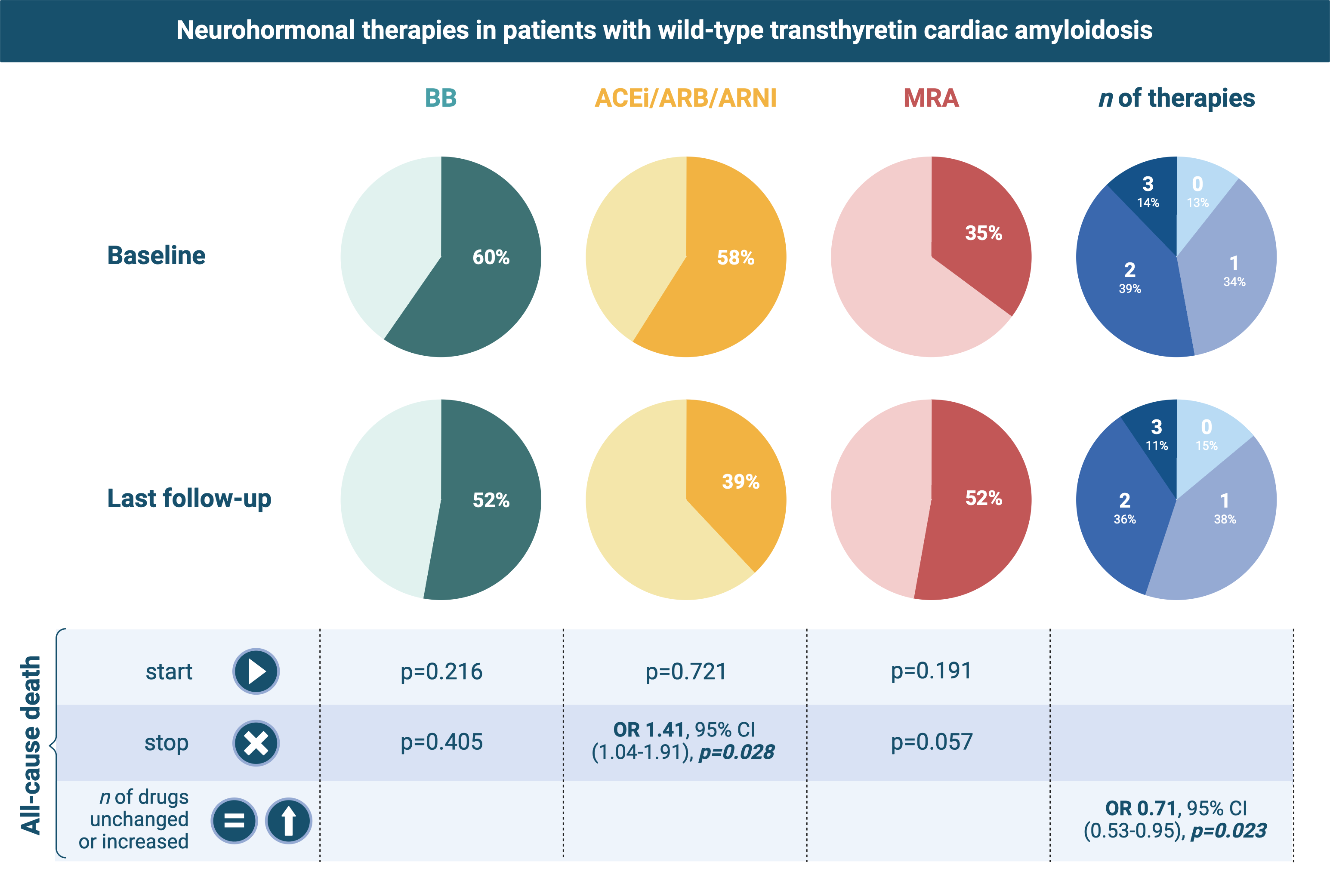
Background: Transthyretin cardiac amyloidosis (ATTR-CA) typically manifests with heart failure (HF). Discontinuing beta-blockers and avoiding angiotensin converting enzyme inhibitors/angiotensin receptor blockers (ACEi/ARB) in patients with ATTR-CA has been recommended. Methods: We investigated the prescription of neurohormonal therapies and their relationship with all-cause mortality in a multicenter cohort. Results: Patients (n=926) had a median age of 79 years (interquartile range 74-83), 90% were men, 17% had a left ventricular ejection fraction (LVEF) ≤40%, and 27% were in New York Heart Association (NYHA) class III/IV. At diagnosis, 60% of patients were on beta-blockers, 58% on ACEi/ARB/ARNI, and 35% on MRA. Patients on beta-blockers had more often NYHA class III/IV, a greater burden of comorbidities, and lower LVEF, and those on ACEi/ARB/ARNI had more comorbidities. Nonetheless, the survival of patients on beta-blockers or ACEi/ARB/ARNI was not significantly shorter over a 2.5-year follow-up (1.6-3.8) (p=0.577 and p=0.977, respectively), and patients on both drugs had not a worse outcome than those not receiving any neurohormonal drug (p=0.575). During the entire follow-up, the number of neurohormonal drugs remained unchanged in 54%, decreased in 27%, and increased in 19%. Patients with a number of neurohormonal drugs either unchanged or increased had a lower risk of mortality (odds ratio 0.71, 95% confidence interval 0.53-0.95, p=0.023). Conclusions: ATTRwt-CA patients on beta-blockers or ACEi/ARB/ARNI at diagnosis did not have a shorter survival. Beta-blockers were discontinued less often than ACEi/ARB/ARNI. There was no sign of better outcomes in patients discontinuing these therapies, or worse outcomes in those starting them.