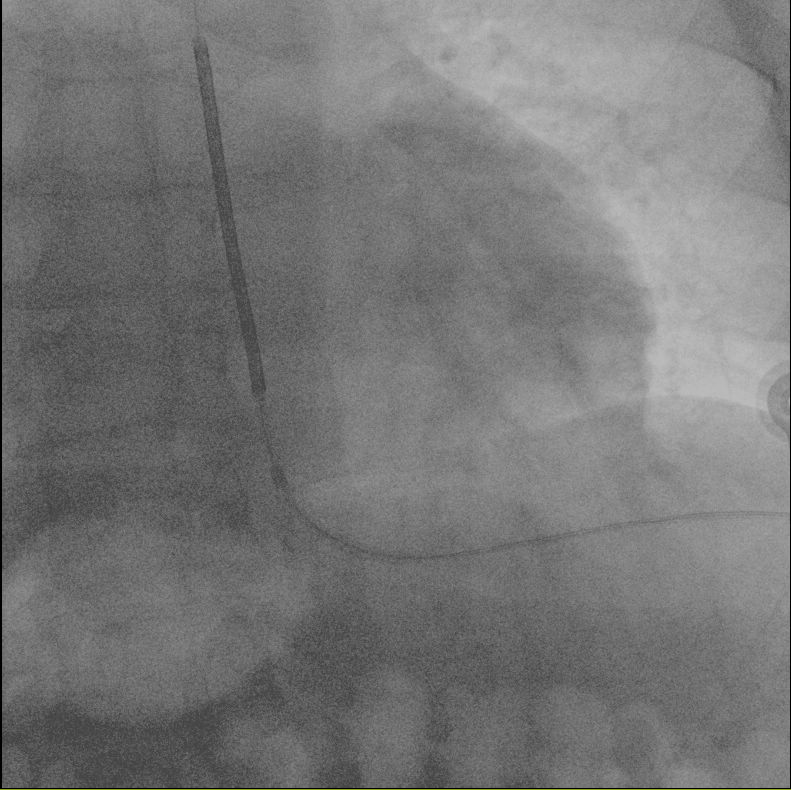
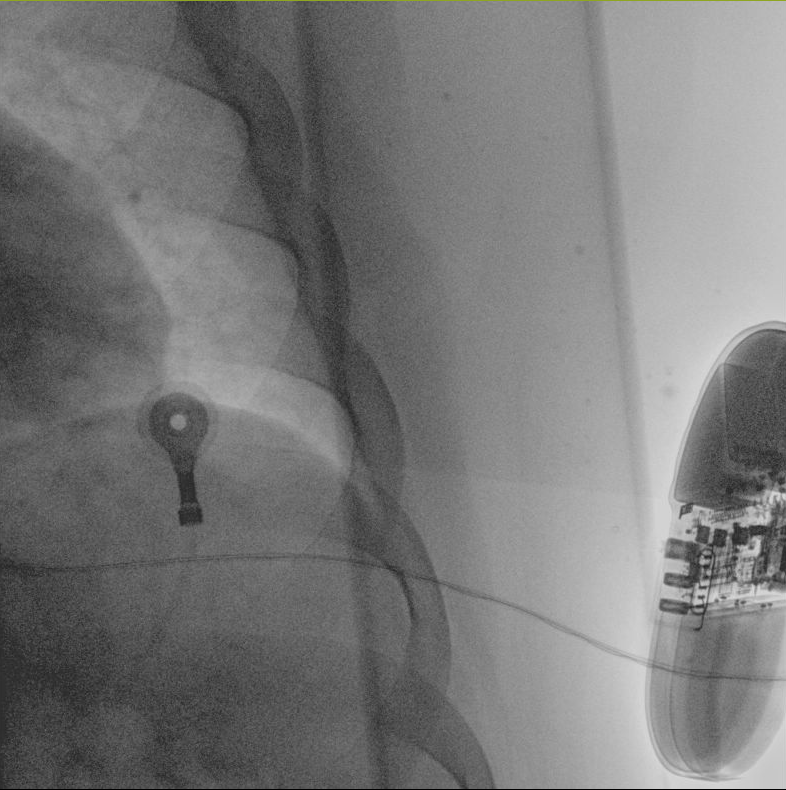
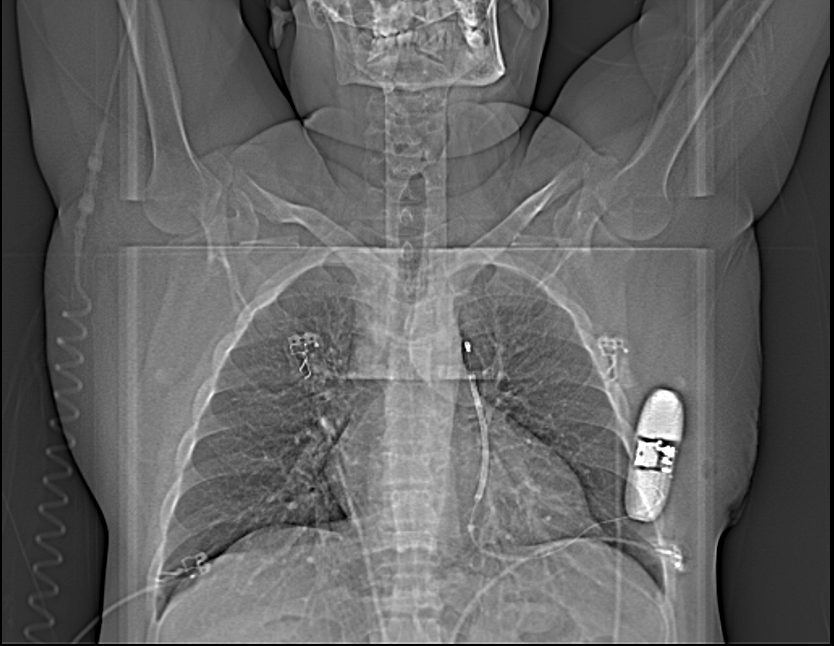
Background: The subcutaneous implantable cardioverter-defibrillator (S-ICD) is becoming increasingly recognized as a first-line choice for patients who are frail or immunocompromised, offering effective protection against sudden cardiac death while minimizing infection risk. Numerous studies, such as the ATLAS and PRAETORIAN randomized controlled trials, have demonstrated that the S-ICD is superior to transvenous ICDs (TV-ICDs) in preventing serious lead-related complications. These findings underscore the S-ICD's advantages in reducing the incidence of infections and invasive lead-associated complications, particularly in vulnerable populations. Methods: We present the case of a 36-year-old male with a history of ischemic cardiomyopathy (CMPD), left ventricular dilatation with severe systolic dysfunction (LVEF 35%), and post-infarction intrastent thrombosis in the left anterior descending artery, treated with angioplasty in October 2024. His medical history was further complicated by thromboembolic disease and a double renal transplant, making him a high-risk candidate for infections. On November 5, 2024, an S-ICD was implanted without complications. The Praetorian score, a validated tool for assessing the adequacy of the S-ICD implantation and an effective alternative to the shock test, particularly in frail patients, was <90, indicating a successful procedure. Results: The implantation was completed without complications, and post-operative follow-up showed no device-related infections or adverse events. The patient’s clinical status remains stable, demonstrating the feasibility and safety of S-ICD implantation in this high-risk population. Conclusions: This case highlights the S-ICD as a viable and effective option for preventing sudden cardiac death in frail and immunocompromised patients, such as those with a history of renal transplantation. The reduced risk of device-related infections makes it particularly suitable for this vulnerable population.