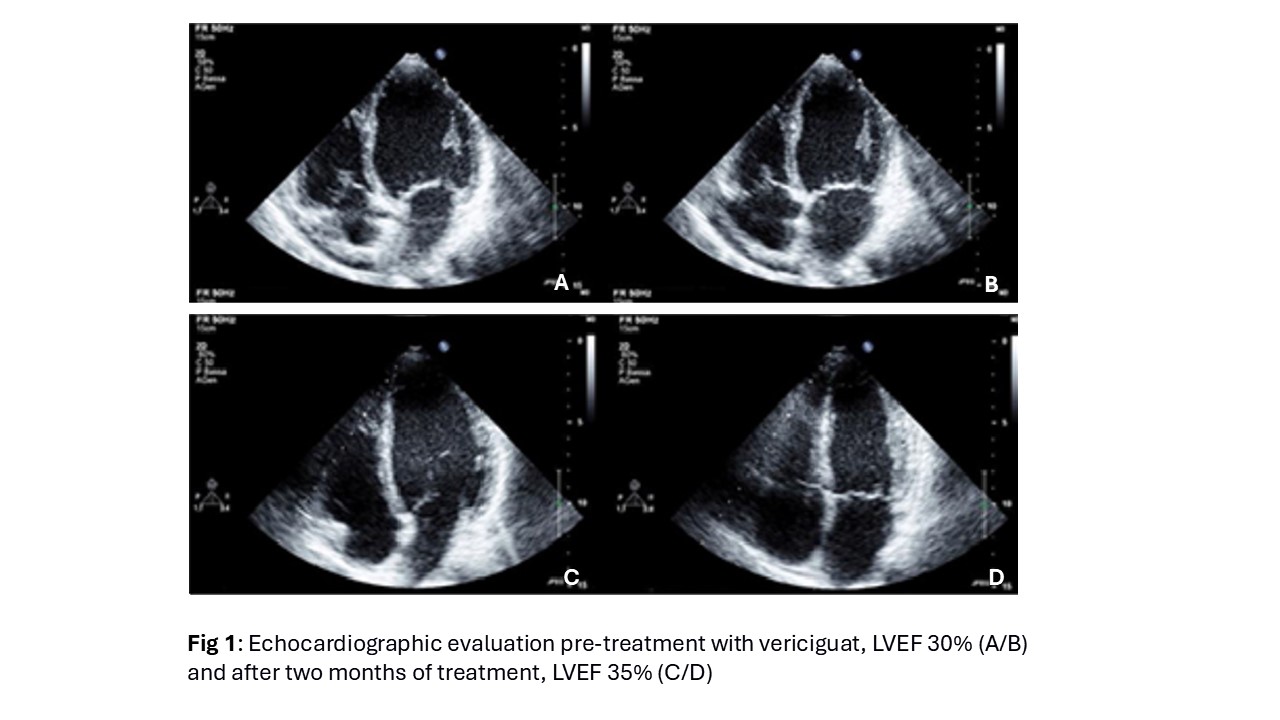
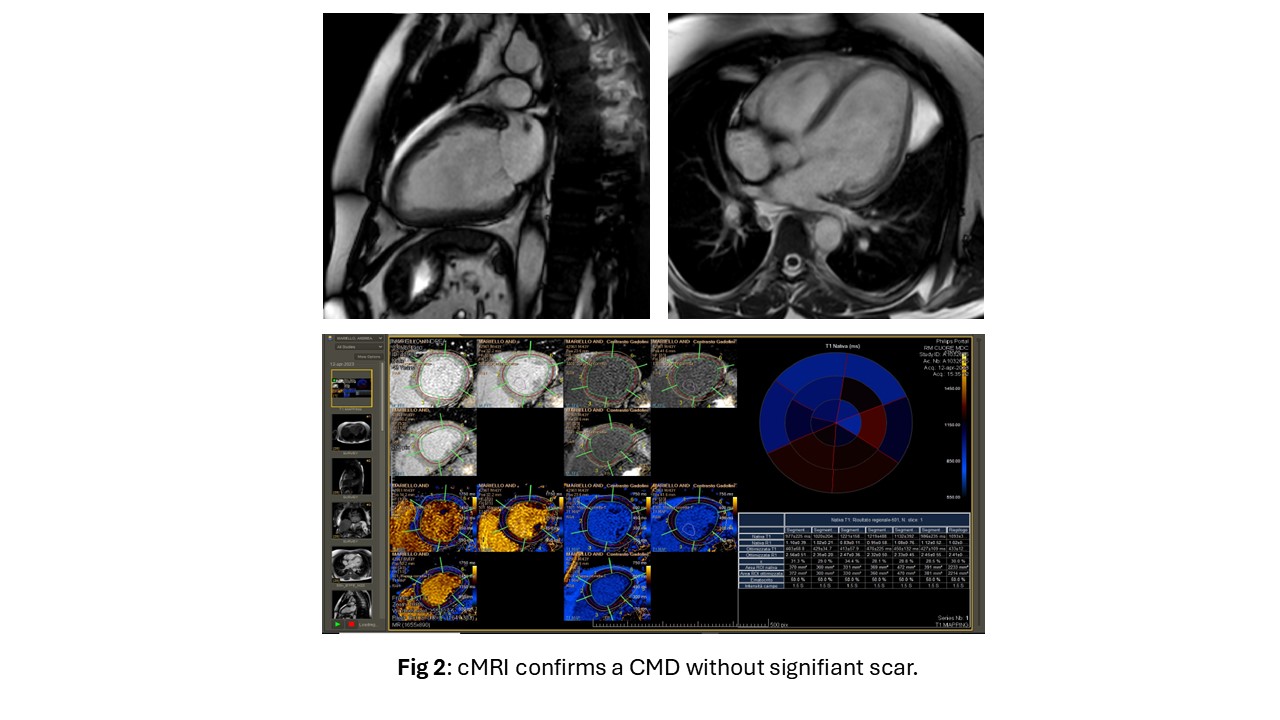
Heart failure (HF) is a syndrome whit complex etiology associated with high mortality and hospitalization risk, despite therapeutic progress. Recent ESC (European Society of Cardiology) guidelines recommend vericiguat use in patients with reduced ejection fraction (HFrEF) with optimal medical therapy and recent episode of HF exacerbation (class IIb). Some recent evidence documents clinical efficacy of vericiguat even in clinically stable patients, but there are no structured studies. Clinical case: A 48-year-old patient with non-ischaemic dilated cardiomyopathy (CMD) comes to our dedicated heart failure clinic for clinical evaluation. On treatment with bisoprolol 5mg bis in die (bid), Dapagliflozin, Ivabradine 10mg bid, Canrenone 25mg. In previous evaluations, intolerance to low doses of ramipril has been detected due to severe hypotension, and moderate reduction in renal function (eGFR 40ml/min/1.73m2). Since the diagnosis of CMD has shown only modest improvement in systolic function; 12/2023 LVEF 28.5% GLS-11.8%, 02/2024 LVEF 29.5% GLS-12.4%, 04/2024 LVEF 30% GLS-12.3% (Fig 1 A/B). Genetic analysis showed no pathogenic mutations. cMRI showed no signs of scar (Fig 2). In May 2024 the implant of dual-chamber implantable defibrillator was performed. To our clinical evaluation, the patient presents NYHA class II. We have introduced vericiguat, up-titrating the dosage to 10 mg, well tolerated. After two months, an improvement of LVEF 35%, GLS-13.3% (Fig 1 C/D), eGFR 44, NT-proBNP 455 pg/ml were observed. The increase of blood pressure allowed the introduction of therapy with valsartan/neprilysin 24/26 bid and increased the dosage of canrenone 50mg. After one month the patient presents NYHA I, and normal blood pressure, and further improvement of NT-proBNP 388 and eGFR 52. In September 2024 LVEF 39% GLS-14%. Conclusions: This clinical case suggests that treatment with vericiguat on top of the optimal medical therapy usually adopted in patients with HFrEF is an effective therapy that can be also recommended in clinically stable patients. The positive effects of treatment can have several favourable repercussions and benefits. In our case, the introduction of vericiguat induced an improvement in systolic function, a consequent increase in blood pressure and an improvement in renal function that allowed the introduction of treatment with well tolerated ARNI and an increase in canrenone dosage, which have amplified the clinical and structural improvement.