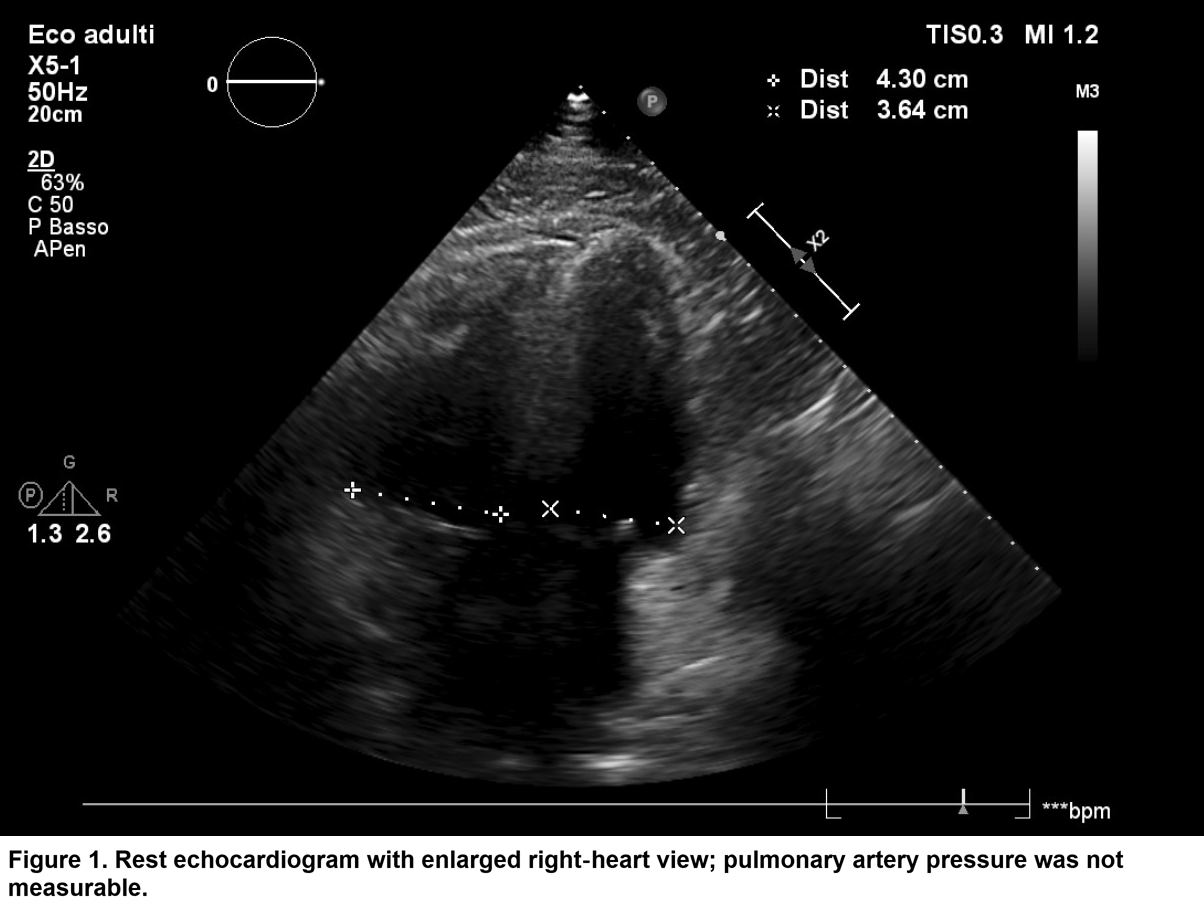
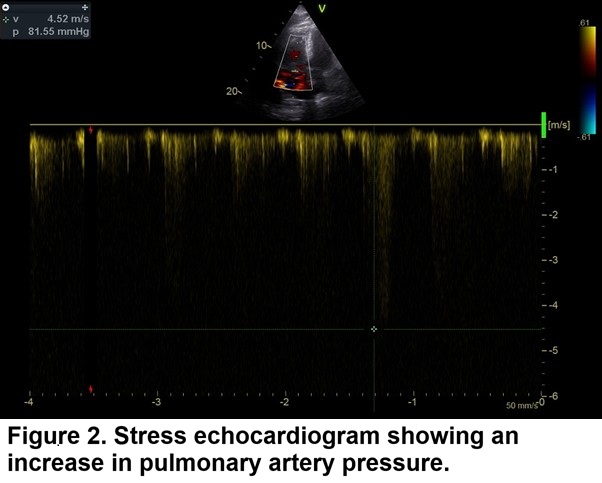
Background Pulmonary hypertension (PH) is a progressive and often underdiagnosed condition that may present with nonspecific symptoms such as exertional dyspnea and fatigue. Its detection is particularly challenging when resting parameters are normal and comorbidities mask early signs. Cardiac rehabilitation offers a unique opportunity to uncover latent forms of PH through structured physical activity and close monitoring. Case Report A 69-year-old man with class III obesity, type 2 diabetes, hypertension, and obstructive sleep apnea syndrome (OSAS) was admitted for chest pain and diagnosed with inferior STEMI. Coronary angiography showed non-obstructive coronary artery disease, consistent with MINOCA. Echocardiography revealed segmental akinesia with preserved LVEF and a dilated but functional right ventricle, with non-measurable pulmonary artery pressures (figure 1). During cardiac rehabilitation, the patient developed exertional dyspnea and significant desaturation during the six minutes walking test, despite normal resting oxygen saturation. Bubble contrast echocardiography suggested a right-to-left shunt on Valsalva, not confirmed on resting TEE. Spirometry revealed mild obstruction; polysomnography confirmed OSAS. Stress echocardiography showed a marked rise in pulmonary artery pressures (PAP 80 mmHg) without inducible ischemia (figure 2). Right heart catheterization demonstrated precapillary pulmonary hypertension with elevated pulmonary vascular resistance (mPAP 30 mmHg, PCWP 11 mmHg, PVR 3.5 WU). Lung perfusion scintigraphy and CT angiography revealed segmental perfusion defects and chronic thromboembolic disease (figure 3), consistent with chronic thromboembolic pulmonary hypertension (CTEPH). Parenchymal findings included emphysematous bullae and ground-glass opacities. The patient was diagnosed with CTEPH and OSAS, representing a rare Group 3–4 pulmonary hypertension overlap. CPAP therapy, Riociguat, and anticoagulation were initiated. Conclusions This case highlights the diagnostic value of cardiac rehabilitation as a clinical observatory for uncovering hidden cardiopulmonary diseases. The structured environment—combining supervised exercise, continuous monitoring, and multidisciplinary assessment—enabled the identification of exertional hypoxemia and led to a targeted diagnostic workup. In patients with unexplained dyspnea, especially those with OSAS, clinicians should maintain a high index of suspicion for pulmonary hypertension.