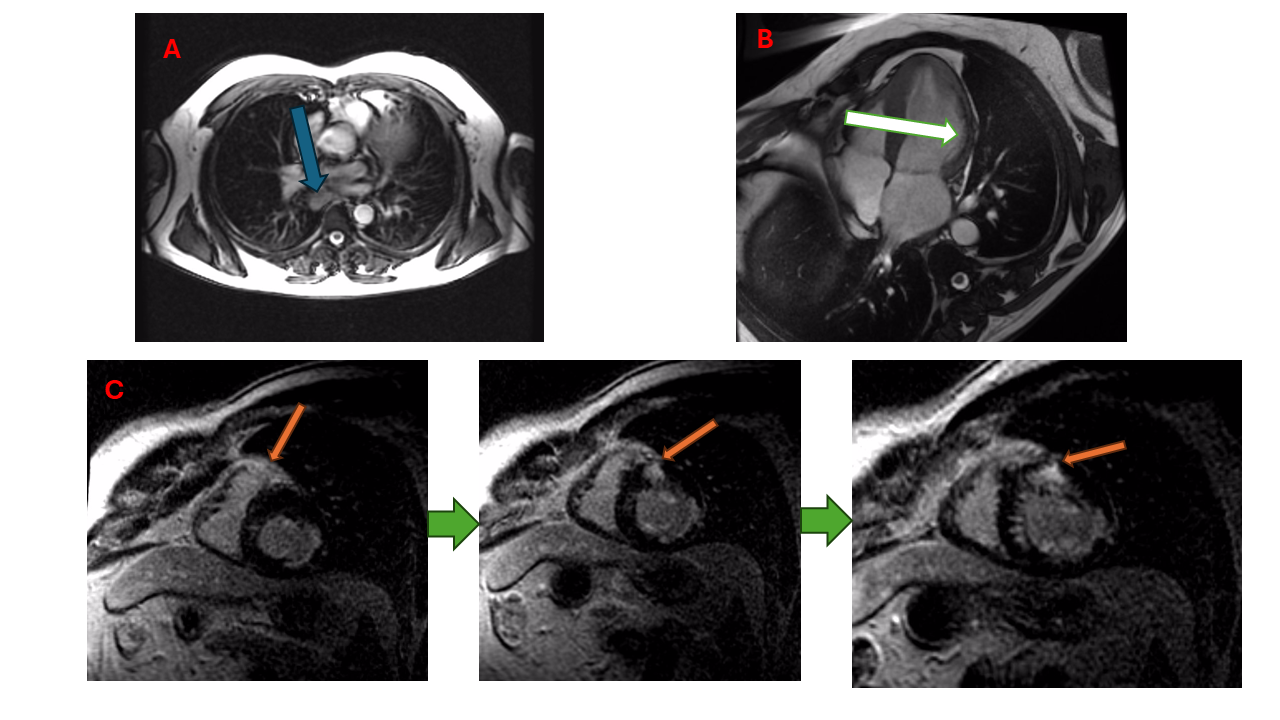
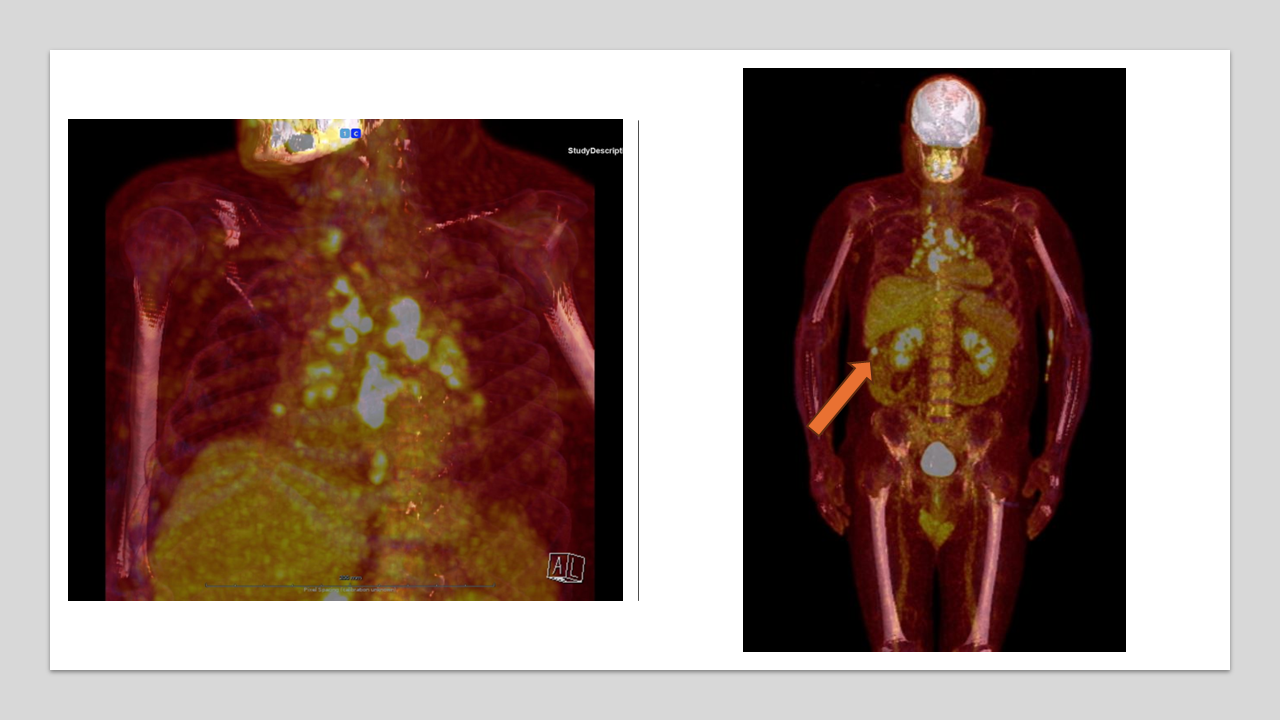
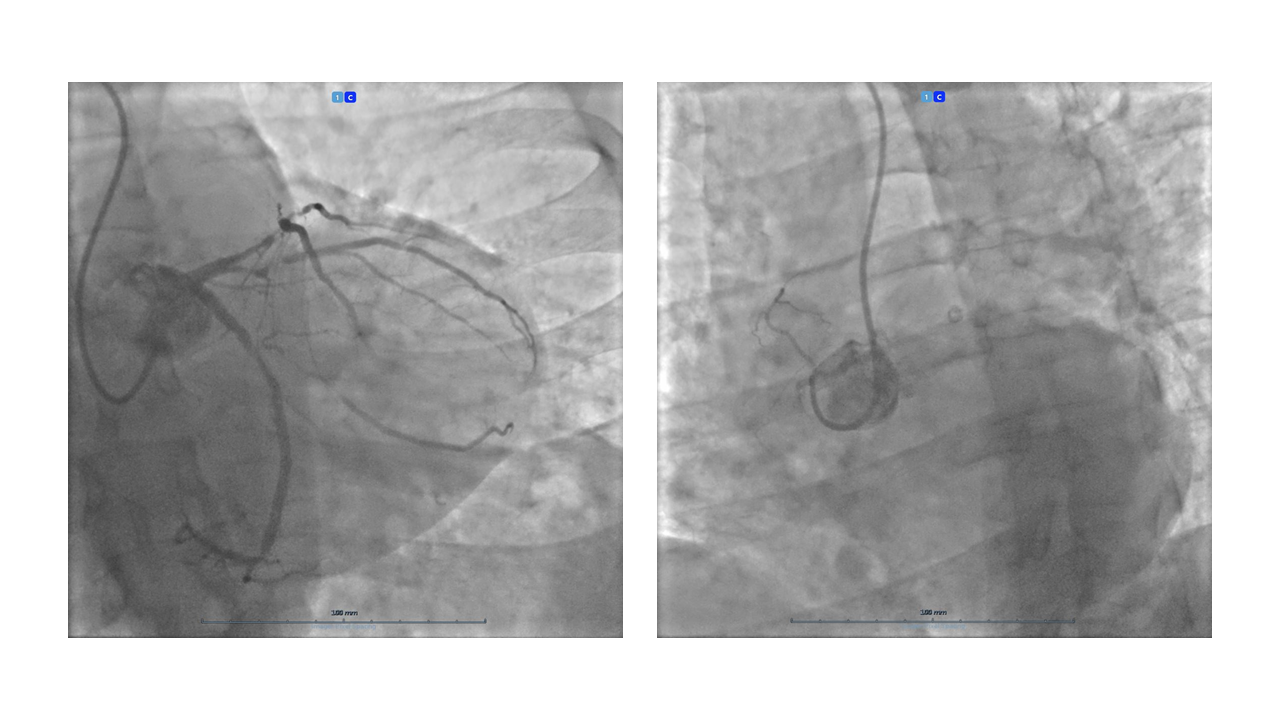
Sarcoidosis is a systemic disease in which a dysregulated immunologic response in genetically predisposed individuals leads to the formation of non-necrotizing inflammatory granulomas Cardiac involvement in sarcoidosis is usually associated with extracardiac sarcoidosis and can present as silent, minimally symptomatic, or clinically manifest. A 44-year-old Caucasian male with an active lifestyle and no cardiovascular risk factors or significant medical history underwent CMR due to a family history of arrhythmogenic cardiomyopathy. Initial localizer images revealed mediastinal lymphadenopathies. Cine imaging showed mild left ventricular dilation and dysfunction, with regional hypokinesia of the lateral wall with fat infiltration. Post-contrast T1-weighted imaging displayed extensive myocardial LGE with a mixed pattern, extending into the right ventricle. Suspecting sarcoidosis, we recommended hospitalization to further assess the risk of active cardiac involvement. Troponin (14 ng/L) and CRP were negative; NT-proBNP was slightly elevated (270 ng/L). A chest X-ray was unremarkable. ECG displayed sinus rhythm at 80 bpm, normal PR and QTc intervals, LBBB and q waves in the inferior leads. Holter ECG recorded 2571 ventricular extrasystoles, but no ventricular tachycardia. Transthoracic echocardiography confirmed mild left ventricular dilation and dysfunction with lateral wall hypokinesia and a normal diastolic function. A thoracic CT scan revealed, multiple mediastinal lymphadenopathies and extensive coronary artery calcifications. An 18F-FDG-PET scan showed intense hypermetabolism in the mediastinal lymphadenopathies. Collaterally, a significant hypermetabolism in the ascending colon suggestive of neoplasia was noted. A subsequent colonoscopy identified a polypoid lesion in the ascending colon, which was removed and confirmed to be high-grade dysplasia on histology. Due to extensive coronary calcifications, a coronary angiogram was performed, revealing severe three-vessel disease. Given his young age, an off-pump coronary artery bypass graft surgery was successfully performed. A follow-up CMR months later showed stable biventricular volumes and function, no edema, and substantially stable fibrosis. The patient was informed about the significant risk of developing life-threatening scar-related arrhythmias. Although the option of an ICD was discussed, he refused. We then decided to implant an ILR and scheduled a three-month follow-up.