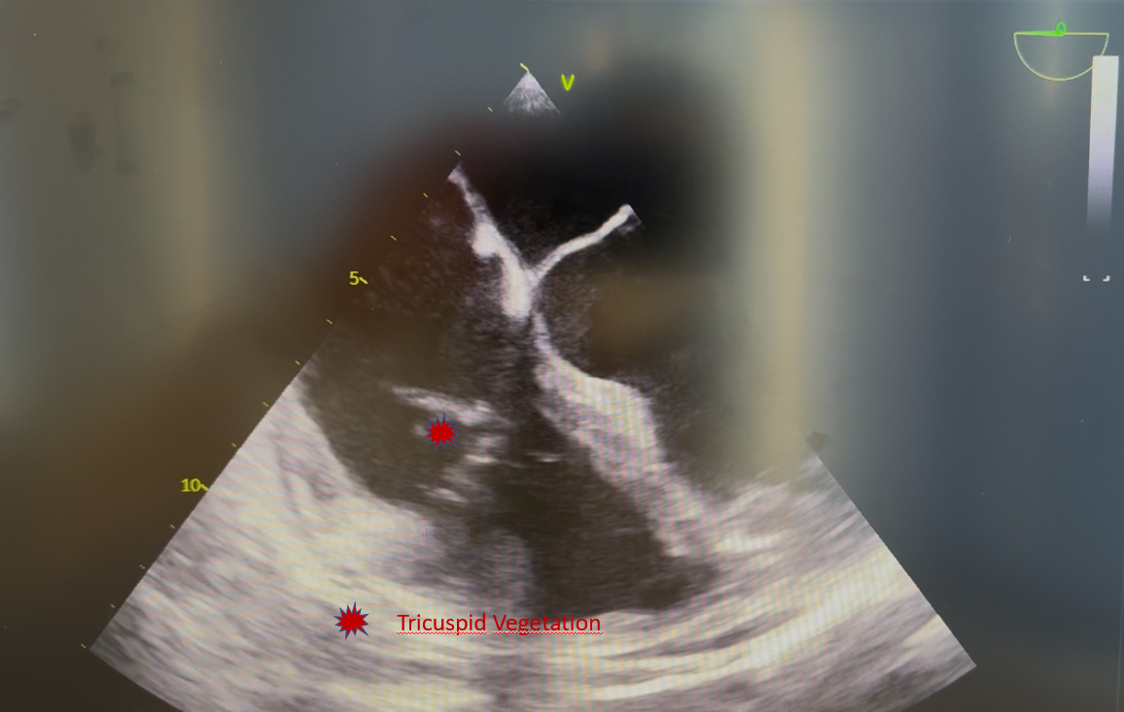
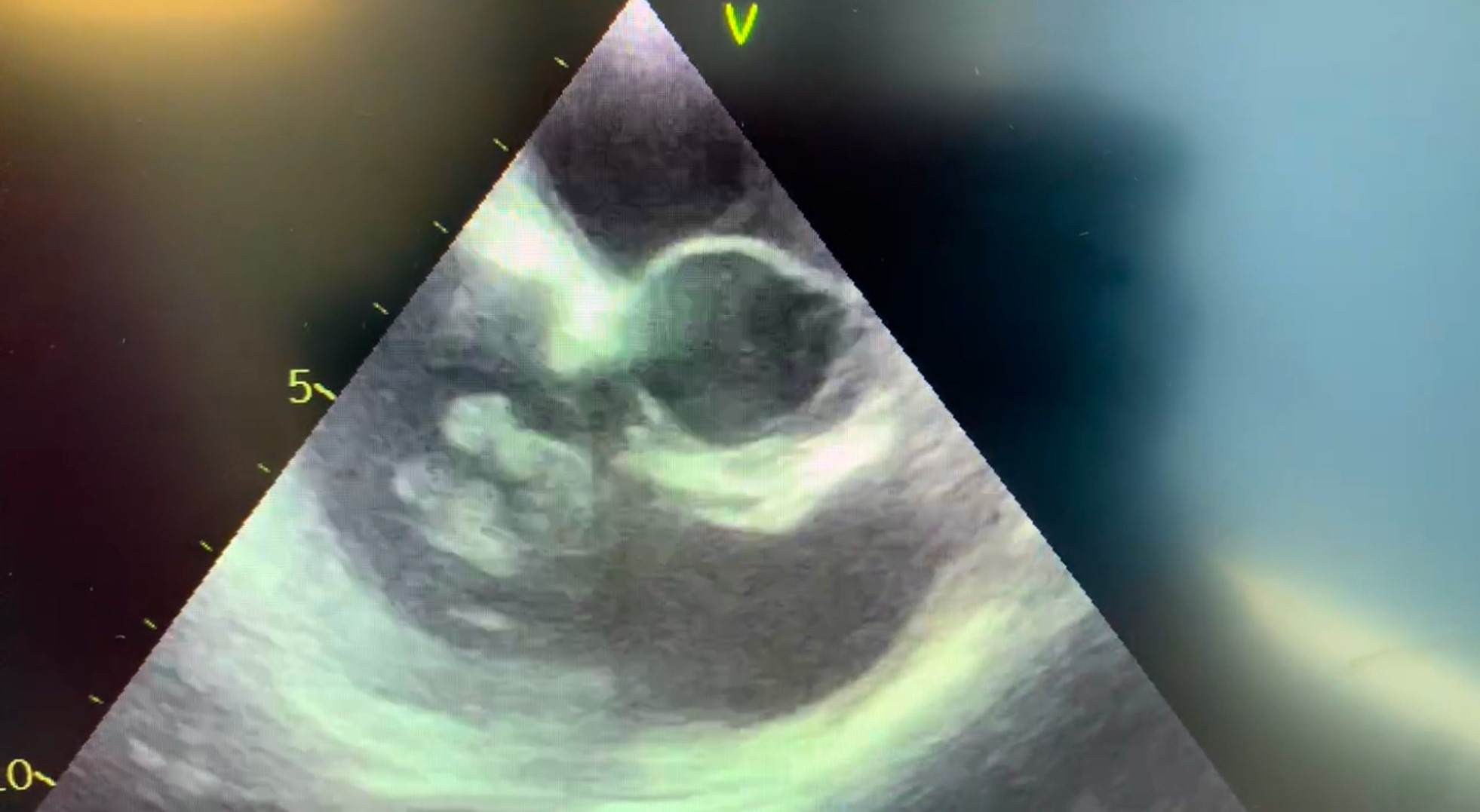
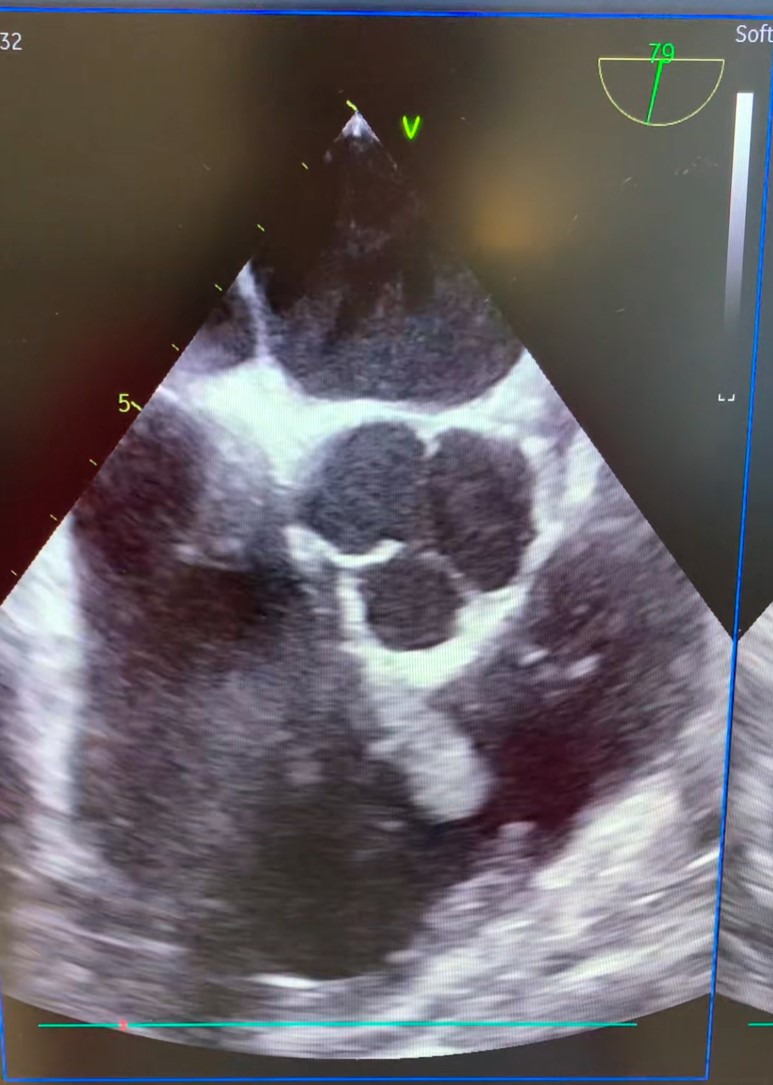
INTRODUCTION: Right-sided infective endocarditis (RSIE) accounts for 10% of all IE cases and affects the tricuspid valve(TV).It is less common than left-sided endocarditis but has distinct clinical characteristic and association.Several mechanisms have been proposed to contribute to RSIE:it mainly affects intravenous drug users(IVDU),but also patients with prosthetic valves,CVC,CIED,congenital heart disease.Due to its rarity and the often nonspecific clinical presentation,RSIE may be underdiagnosed or delayed in diagnosis,leading to potential complications such as severe valvular regurgitation(VR),septic embolism and HF. AIM: this case series highlights the clinical course,diagnostic approach and management of a patient with RSIE,emphasizing the importance of TOE in early recognition and appropriate treatment to prevent severe complications. METHODS: from March to Nov 2024 we diagnosed 5 cases of RSIE.All patients underwent to TTE and TOE.Blood cultures were performed in all of them.The patients were classified based on sex (4m,1f),age,risk factors(IVDU,immunosuppression,lead infection),pathogen,vegetation size,presence of septic pulmonary emboli,presence of vegetation on TV,antibiotic therapy,need for surgery,outcomes. RESULTS: majority of patients were IVDU;lead infections and immunosuppression were also identified as risk factors.Staph.Aureus(MSSA)was the predominant pathogen;K.Pneumoniae was seen in one patient.Common symptoms included fever(100%),dyspnea and arthralgias.Septic pulmonary emboli were present in 80% of cases.All patients had vegetations on TV at ETT,except one patient.VR were moderate-to severe in all cases,with preserved right ventricular function.Vegetation sizes ranged from 12 to 23mm.All patients underwent to TTE and TOE;none of them required surgical intervention.All the patients recovered,highlighting the efficacy of timely medical management. DISCUSSION: in the majority of patients,TTE was diagnostic,but in one patient was not decisive:in this patient,despiteTTE was quite normal and blood cultures were negative,TOE was performed for high clinical suspicion of IE and showed vegetation on the tricuspid valve,thus confirming its usefulness. CONCLUSIONS: in our experience,TOE is mandatory in allowing a timely diagnosis of RSIE even in the absence of TTE positivity or positivity of blood cultures,thus allowing an early start of targeted antibiotic therapy ensuring therapeutic success.