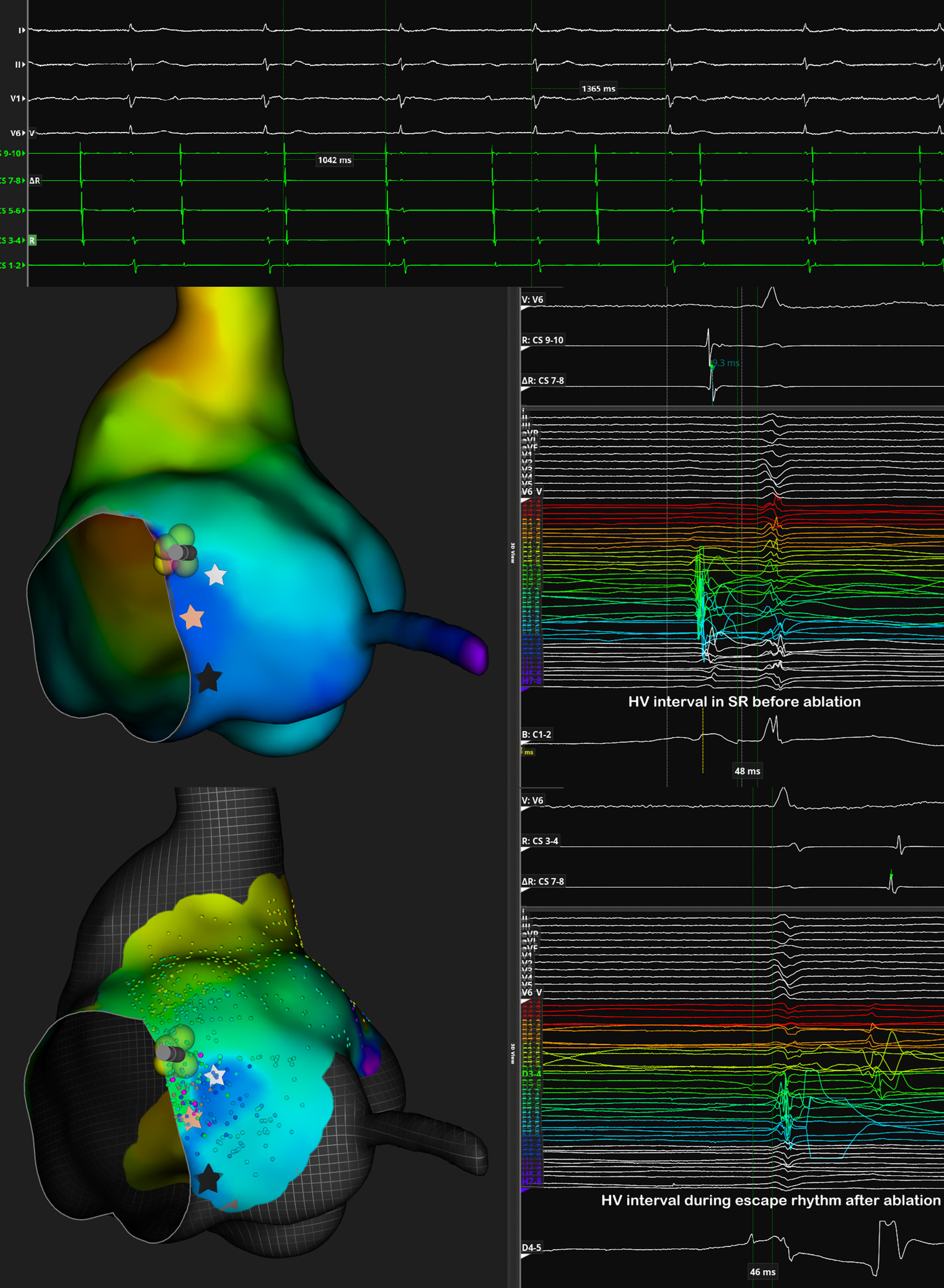
Background: Atrioventricular (AV) junctional ablation is commonly performed to treat refractory arrhythmias by disrupting AV conduction. The procedure traditionally targets either the site with the earliest His bundle potential or the most prominent His potential. However, this could lead to a proarrhythmic risk linked to QT interval prolongation and heightened QT dispersion shortly after His potential ablation. Performing ablation on the compact AV node potential could be equally effective, improving response safety and reducing arrhythmic risk. We report the case of a patient who underwent ablate and pace ablation using the direct recording of the AV nodal potential. Methods: Compact AV node location was determined by high-density mapping performed with a multipolar basket catheter. The AV node extracellular potential recorded resulted in a low-frequency, hump-shaped, low amplitude, slow waveform, long duration electrogram. Radiofrequency ablation was performed specifically over the electrogram recognized as compact AV node potential. Results: The procedure was completed by applying radiofrequency energy to the recording site of the compact AV node. The radiofrequency ablation induced a rapid and complete AV block. This block was characterized by the occurrence of fast, non-retroconducted junctional beats. The resulting block was intranodal, as indicated by the emergence of a narrow QRS complex and junctional rhythm with a rate of approximately 45 beats per minute. The QRS morphology remained identical to that of conducted beats observed before ablation. Post-ablation recordings of the His electrogram revealed a distinct His potential preceding the QRS complex, with an HV interval consistent with pre-ablation measurements. Additionally, no Hisian potential following the atrial electrogram was recorded. Conclusions: Anatomical ablation of the AV node potential has proven to be both feasible and safe, producing an escape rhythm comparable to the pre-ablation rhythm and achieving an effective conduction block while minimizing the risk of proarrhythmic complications.