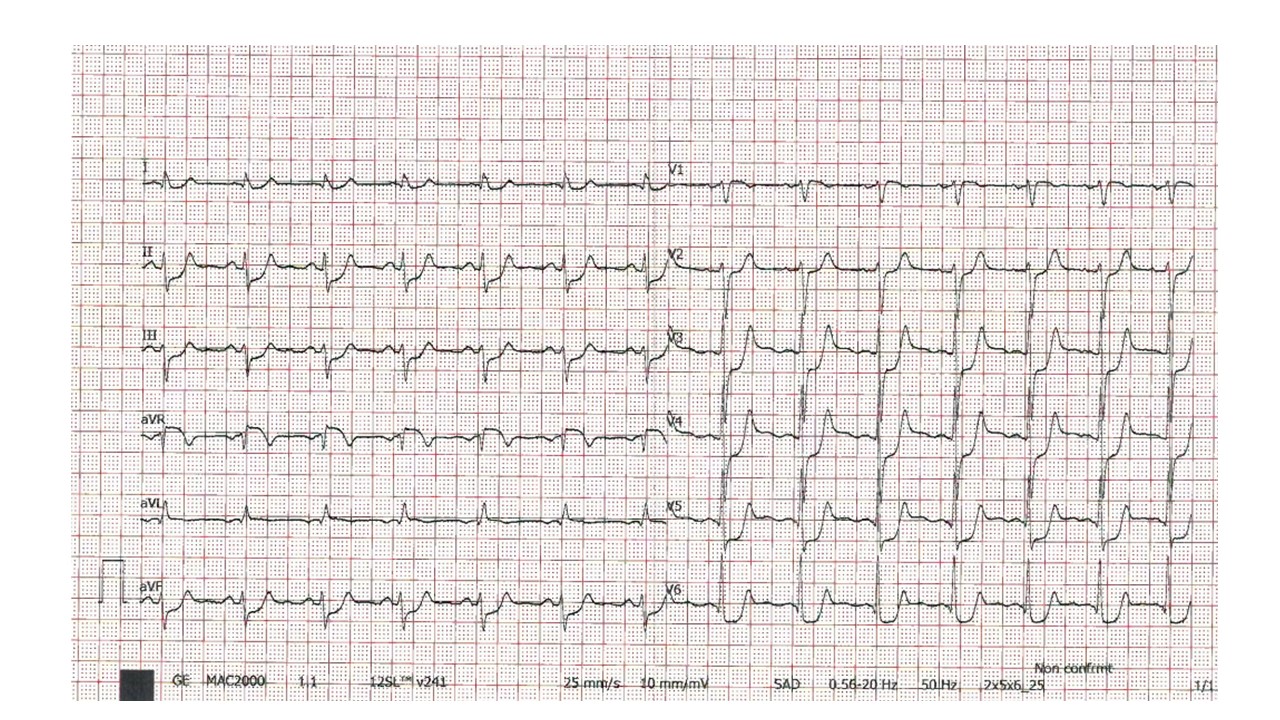
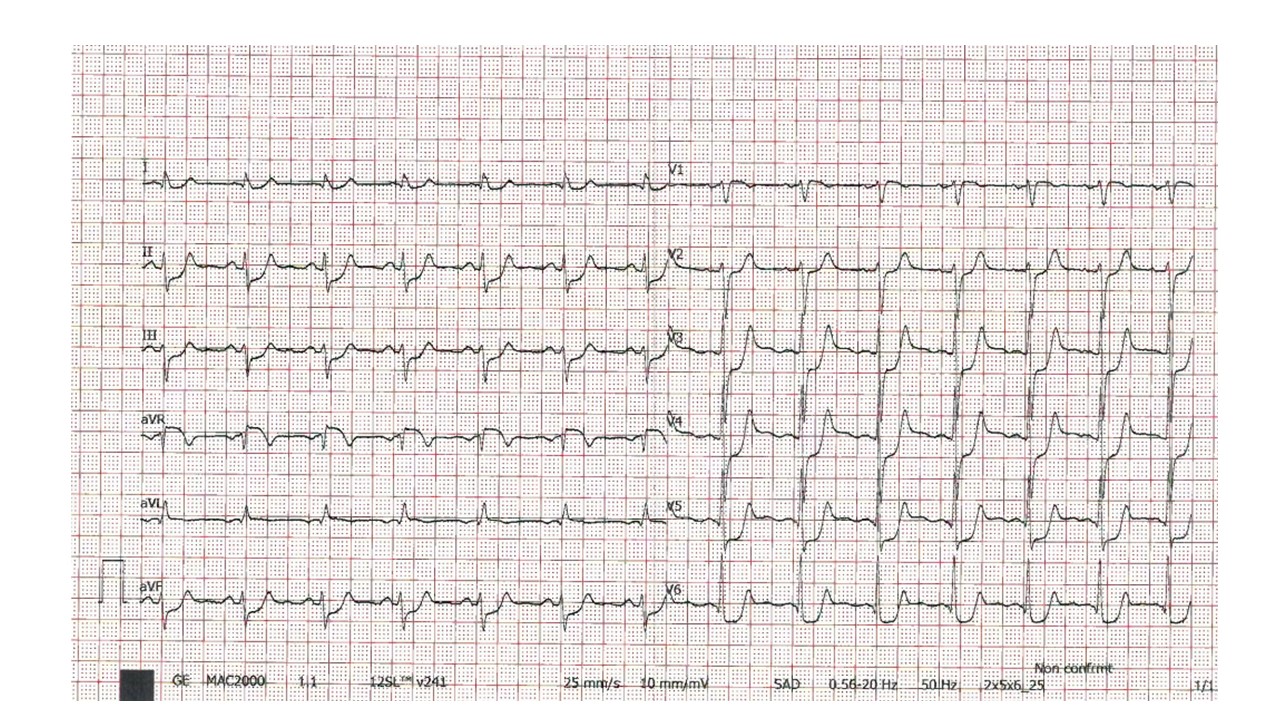
Changes in repolarization resulting from a brief period of atypical ventricular activation are called cardiac memory (CM). When this abnormal activation ceases, the repolarization (T wave) vector aligns with the vector of the "abnormally" activated QRS complex. In leads where the prior "abnormal" QRS complex was negative, CM presents as T wave inversions, while in leads where the prior "abnormal" QRS complex was positive, T waves are observed . CM is associated with various heart diseases, including ventricular paced rhythm, PVC, intermittent left bundle branch block, ventricular tachycardia, and Wolff-Parkinson-White syndrome . Few reported ST-segment elevation cases exist in the context of "cardiac memory.” This could be the first documented case of "cardiac memory" presenting as ST elevation following reentrant supraventricular tachycardias. With this clinical case, we want to emphasize the possibility of an ST-segment memory, like a T-wave memory. A 47y old man presented to our emergency department complaining tachycardia and chest discomfort. He had no medical history. An ECG at admission showed wide QRS tachycardia with a heart rate of 205 beats per minute (fig1) The tachycardia spontaneously regressed during the evaluation. However, at the follow-up ECG, there was diffuse ST-segment depression with a supra-sloped ST at AVr, regretted within the next 25 minutes (Fig 2-3) Considering the uncertain situation, the patient was admitted to the cardiology department. Coronary angiography was performed to rule out any damage to the coronary arteries. No signs of thrombus, dissection, stenosis, or vasospasm were observed. An electrophysiologic study was performed during the same hospitalization, which showed evidence of orthodromic atrioventricular re-entry tachycardia conducted with aberrancy to the left bundle branch block through a posteroseptal accessory pathway, which was later ablated.We believe these irregularities were a form of ST-segment cardiac memory, as there was no other logical explanation for the ST elevation. Furthermore, the fact that these anomalies disappeared within a few hours and the results of the tests conducted support the possibility that CM is responsible for the ST-segment elevation in our patient.