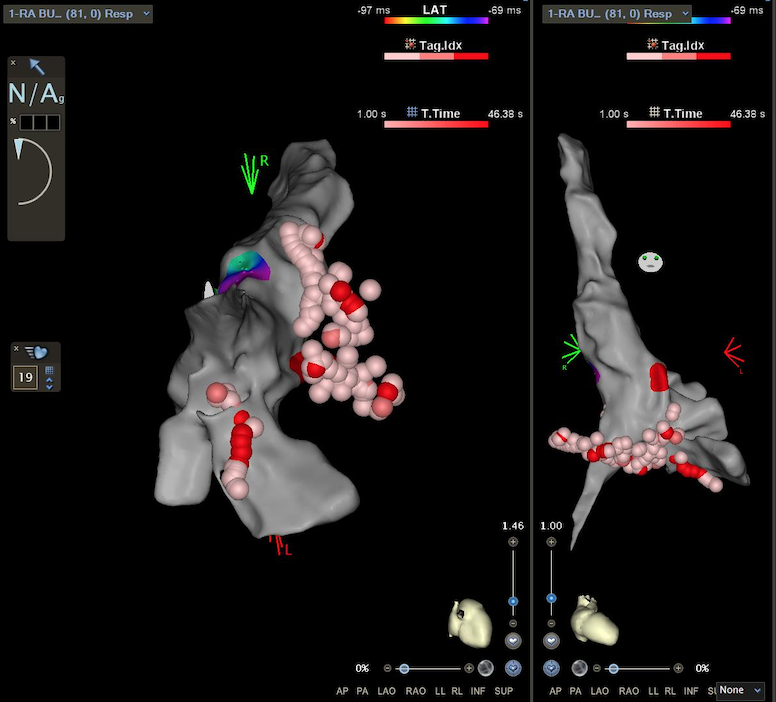
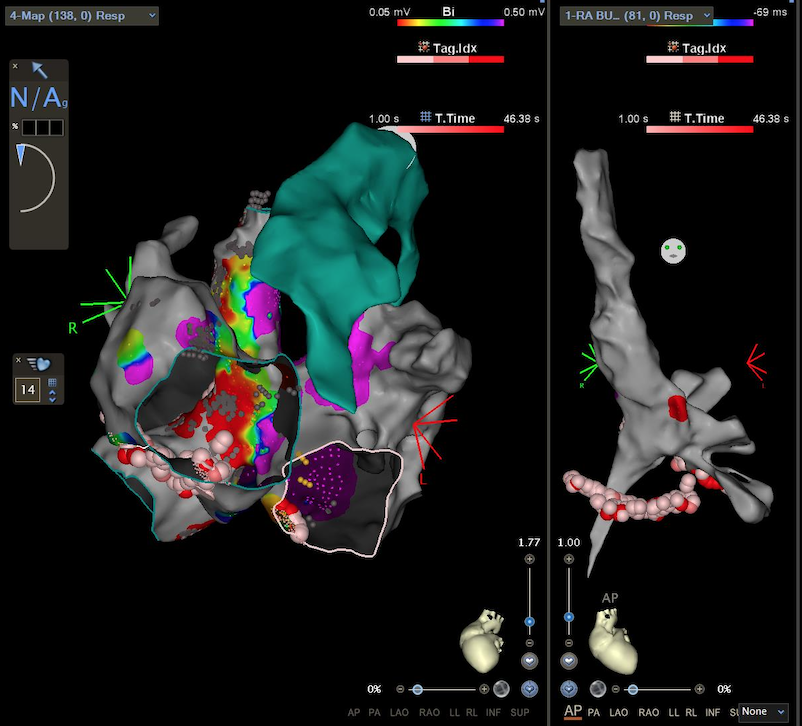
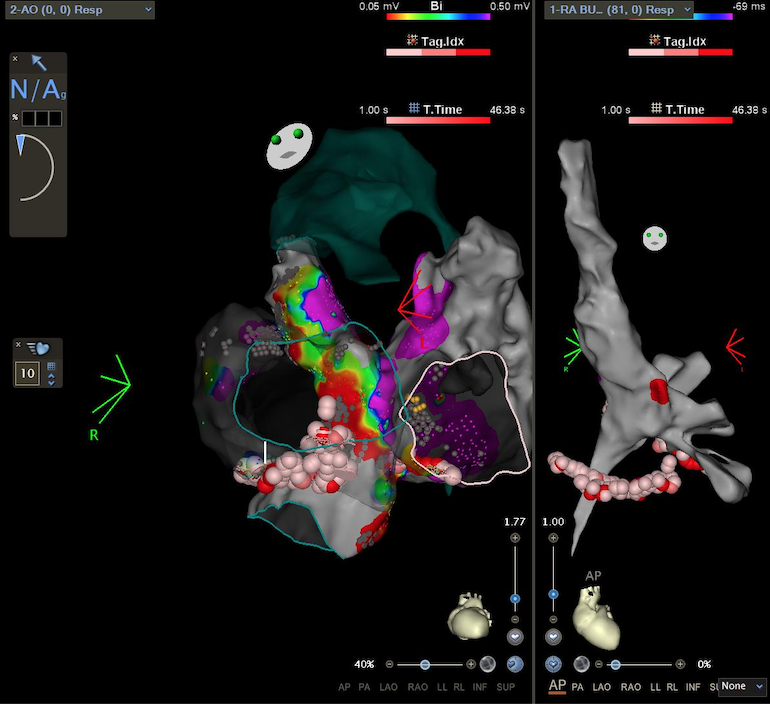
A 33-year-old male with dextro-transposition of the great arteries and an interventricular septal defect underwent congenital heart surgery using the Senning procedure and patch closure. Consequently, he developed sinus node dysfunction, resulting in bradycardia and a poor response to exercise. Successive medical history has been characterized by multiple episodes of supraventricular tachycardia treated with electrical cardioversions (ECV) and transcatheter ablations. In 2021, the first ablation aimed at a cavotricuspid isthmus-dependent atrial flutter. The procedure failed due to the incapacity of catheter positioning in the isthmus region via the retrograde transaortic approach. In 2022, the patient underwent a second procedure for arrhythmia recurrence. Activation mapping of the pulmonary venous atrial system revealed centrifugal activation at the left atrial patch's basal segment. Despite attempts to target a fragmented line at the venous suture with radiofrequency (RF) delivery, the arrhythmia persisted, and the detached baffle could not be accessed. Retrograde mapping of the arterial atrium showed improved precocity of the arrhythmia critical isthmus. A single RF delivery successfully abolished the arrhythmia. In August 2024, the patient had a relapse of atrial tachycardia with hemodynamic instability, treated with ECV. Beta-blockers, amiodarone, and sotalol failed to prevent further arrhythmias. A redo ablation attempt was made. Due to the challenging cannulation of the coronary sinus, we utilized a quadripolar transesophageal lead as an atrial reference. An electroanatomical map of the right atrial chamber identified two areas of slowed conduction: one at the free wall of the right atrium and another at the cavo-mitral isthmus. An ablation line was performed at these levels—the inter-caval and the sub-pulmonary cavo-mitral isthmus. The systemic atrial chamber was accessed via a retrograde aortic approach. The activation map revealed the presence of peri-tricuspid re-entry. We performed an RF delivery between the inferior valve anulus and a posterior silent region toward the left atrium. This procedure successfully interrupted the arrhythmia and restored RS. The patient's clinical course has been stable, with a consistent sinus rhythm, and dismissed with beta-blocker therapy. The challenges in identifying and managing compicated arrhythmias are emphasized in this clinical case, due to complex heart anatomy