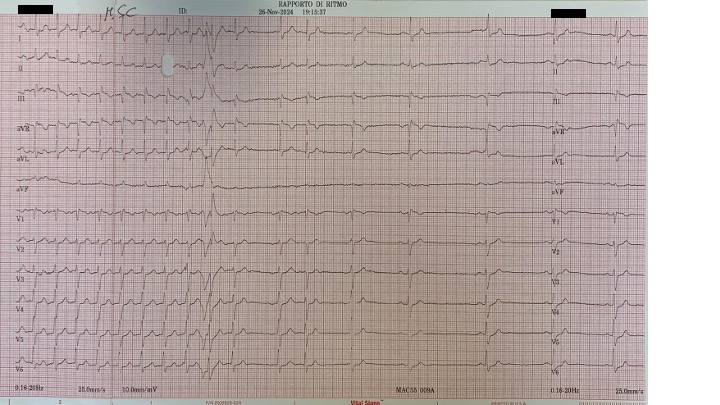
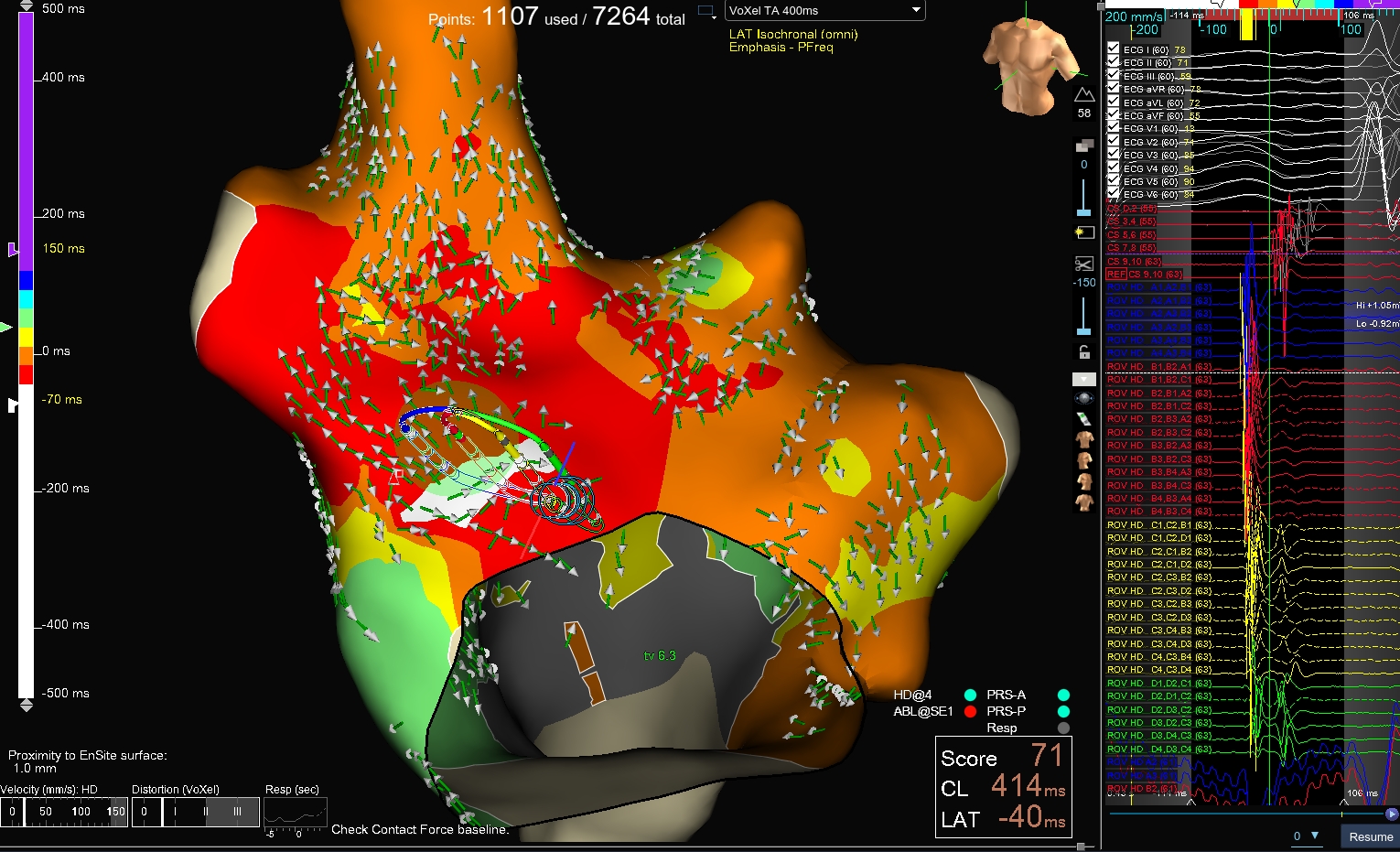
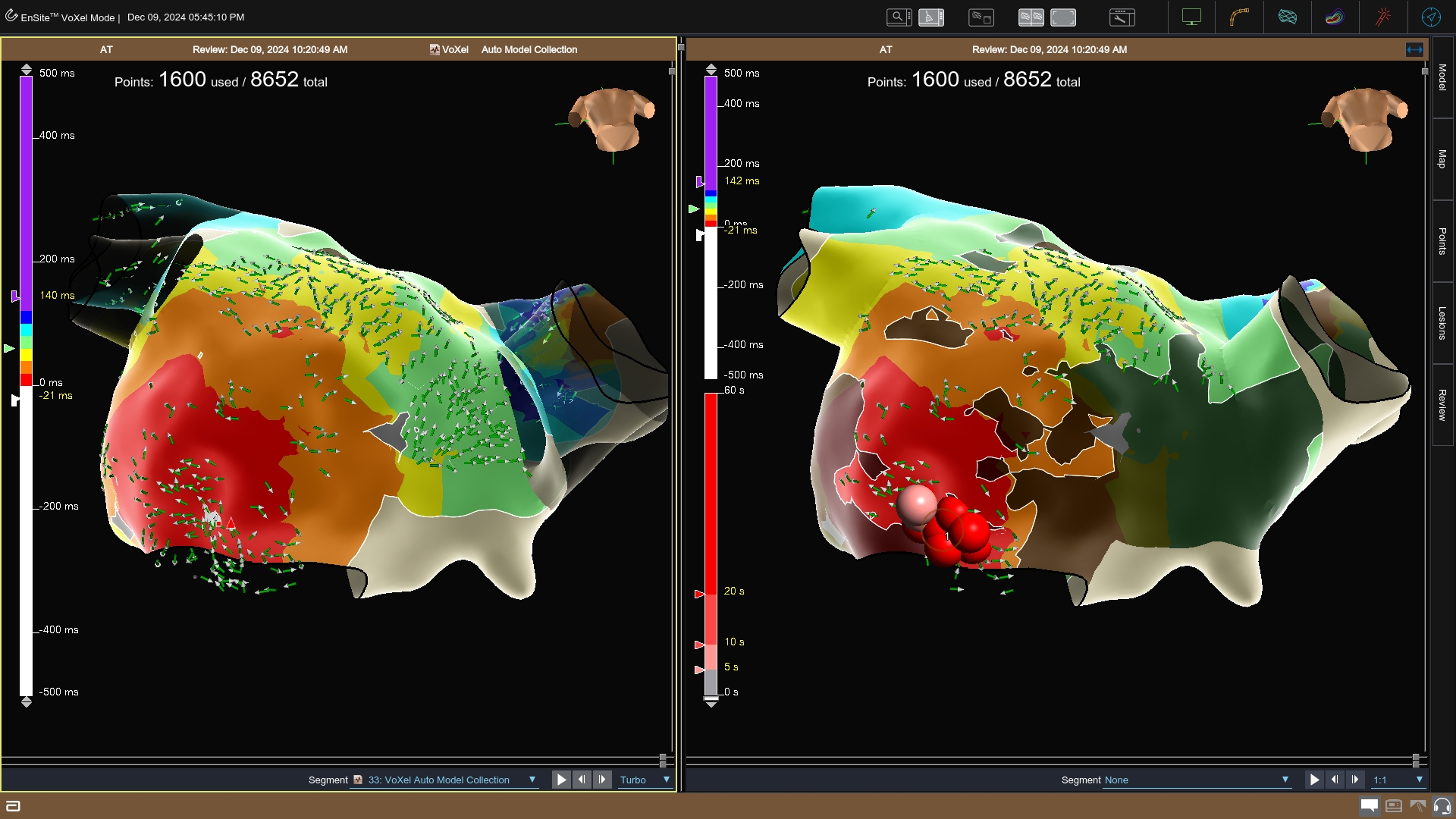
Here we report two cases of a 79-yo diabetic and hypertensive male and a 58-yo hypertensive female patients with similar clinical features: both suffered from frequent recurrent episodes of paroxysmal supraventricular tachycardias, sensitive to vagal maneuvers and adenosine. They were referred to catheter ablation because the arrhythmia recurred despite medical therapy with beta-blockers and/or flecainide. The electrophysiological study showed similar characteristics: the arrhythmia was easily inducible during stimulation with a induction pattern V-A-A-V and interrupted by overdrive pacing; it was not inducible during isoproterenol infusion. These features suggested a mechanism related to triggered activity. An activation map was then performed and showed focal atrial tachycardia arising in the first case from the antero-lateral portion of the tricuspid annulus, while in the second case from the postero-lateral portion of the mitral annulus. RF delivery up to 35 W interrupted the arrhythmias, that were no longer inducible. Triggered atrial tachycardias are due to late post-depolarizations, which are made up of low voltage oscillations at the end of the action potential. These oscillations are favored by the flow of calcium ions into the myocytes. If these oscillations are of sufficient amplitude to reach a certain threshold of action potential, a new depolarization is triggered. If the phenomenon is single, it will give rise to an extrasystole, if recurrent, it will result in sustained tachycardia. It can respond to measures such as vagal manoeuvres or medications such as adenosine, verapamil or beta-blockers by increasing the refractory period of the myocardium. The criteria used for the diagnosis are:1)induced by programmed or decremental atrial stimulation;2)Atrial pacing, cycle length and the coupling interval of atrial extrasystoles are directly related to the interval of onset of tachycardia;3)P-R is related to the frequency of tachycardia;4)The degree of blockage of the tachycardia does not affect the cycle;5)acceleration of AT during overdrive is also typical. In conclusion, these two cases showed a peculiar association of triggered atrial arrhythmias and the region of the fibrous skeleton of the heart, particularly the region of the mitral and tricuspid annuli. The reasons is unclear but could be probably related to the tendency of the transition cells hereby located to develop a calcium overload that can ultimately lead to such arrhythmias.