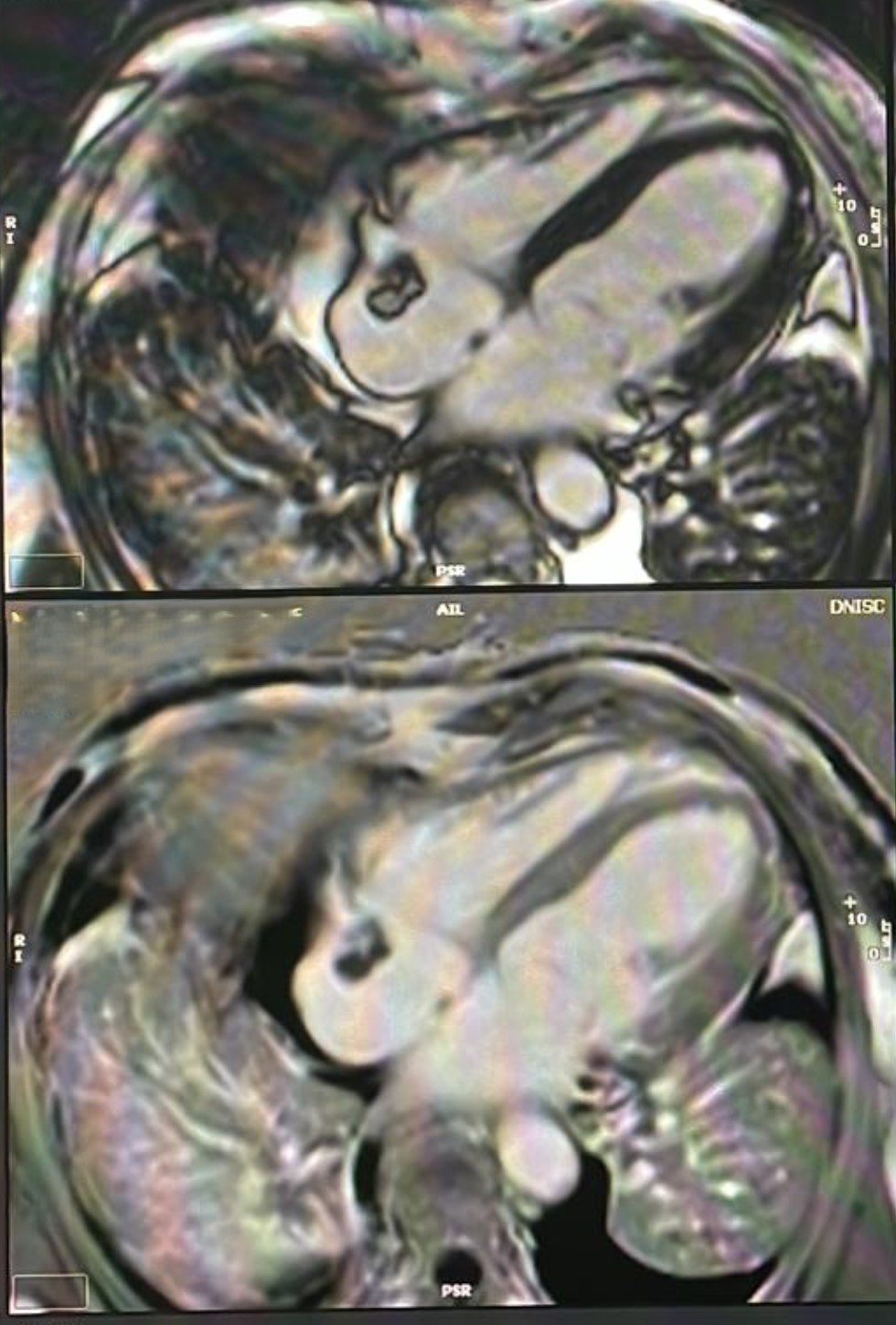
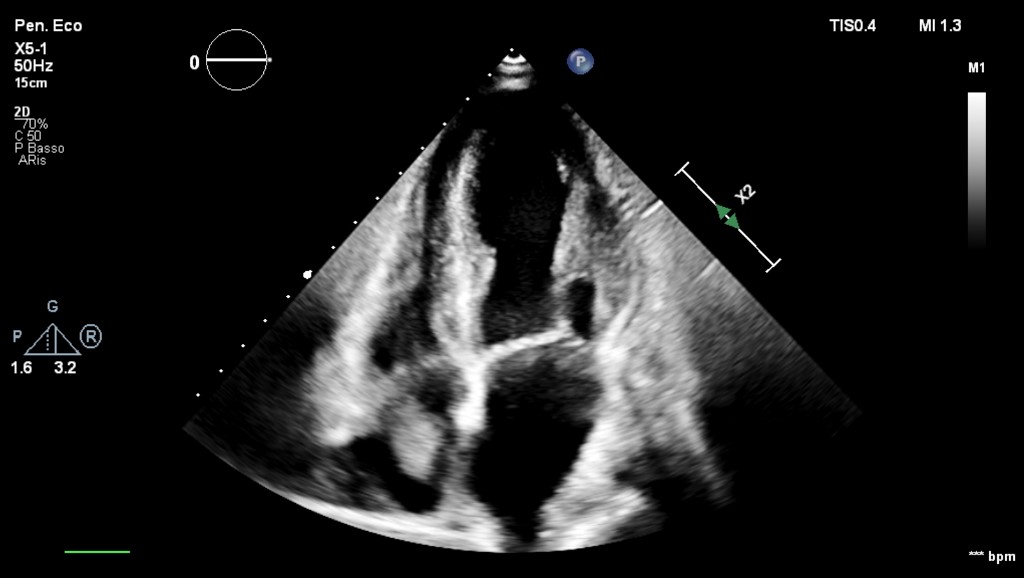
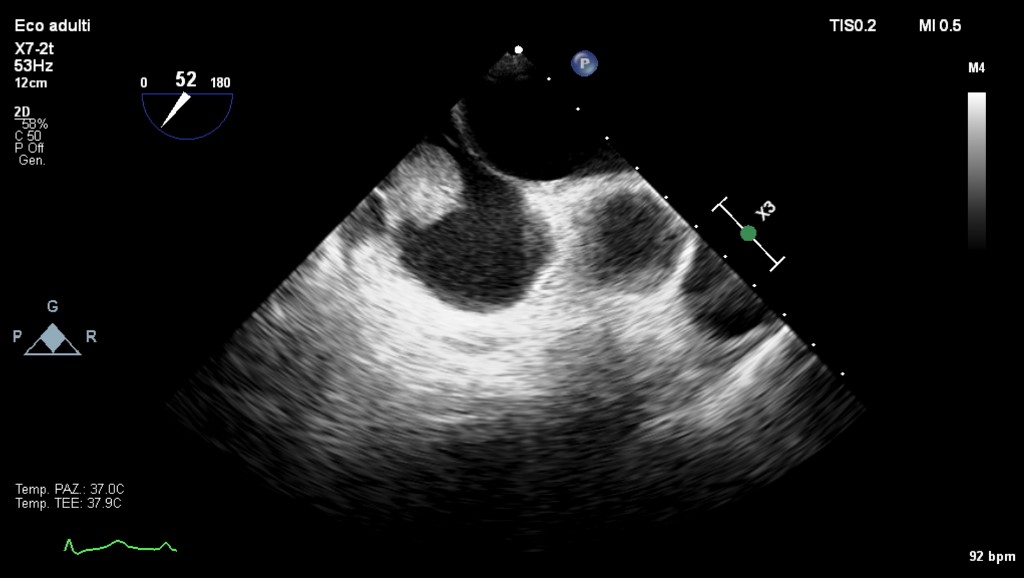
A 65-year-old woman presented to the emergency department with fever for several weeks. The patient had a history of hypertension and chronic renal failure, currently undergoing renal replacement therapy via dialysis using a central venous catheter placed in the right internal jugular vein. Blood tests revealed a marked increase in white blood cells and inflammatory markers (CRP 150, procalcitonin 40). Hemodynamic parameters were stable. Chest radiography showed atelectasis in both lung bases, consistent with pneumonia. An echocardiogram was performed: non-dilated left ventricle, concentric wall hypertrophy, a global ejection fraction of 50% due to hypokinesia of the inferior wall, which was also hyperechoic and thinned; moderate degenerative mitral insufficiency; aortic dimensions within normal limits; and an iso-echoic mass in the right atrium, likely pedunculated and attached to the roof, measuring approximately 2.5 cm x 2 cm, with no impact on right ventricular inflow. Suspecting an endocarditic lesion, the patient was admitted to cardiology, and the central venous catheter was promptly removed, with the tip cultured, which returned negative results. However, blood cultures were positive for Staphylococcus epidermidis. A transesophageal echocardiogram confirmed the presence of a pedunculated mass in the right atrium, attached near the superior vena cava junction, suggestive of thrombosis or endocarditis. Cardiac magnetic resonance imaging was performed, showing early and late peripheral contrast enhancement, ruling out thrombosis and endocarditis, and suggesting the possibility of a primary cardiac mass, particularly a myxoma, or cardiac metastasis. A whole-body PET-CT scan was then conducted, which showed no pathological uptake indicative of tumors throughout the body or infectious processes in the heart, confirming the inferior wall hypokinesia with ischemic-type late gadolinium enhancement. The diagnosis of right atrial myxoma was thus confirmed. The patient continued targeted antibiotic therapy based on the antibiogram until the inflammatory state resolved. She is currently awaiting coronary angiography for further diagnostic and therapeutic management. This clinical case highlights the importance of multimodality imaging in the study of intracardiac masses, leading to a diagnosis that was entirely different from the initial clinical presentation. Right atrial myxoma is a rare manifestation, entirely atypical in this clinical context.