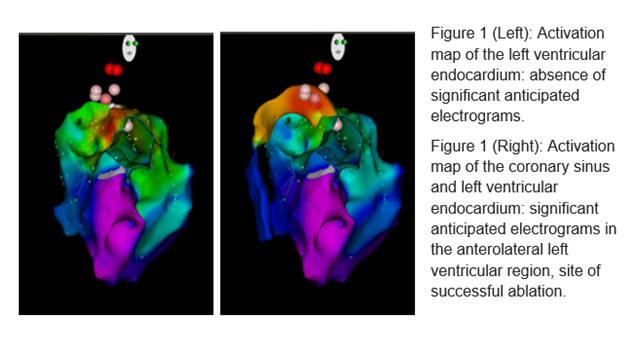
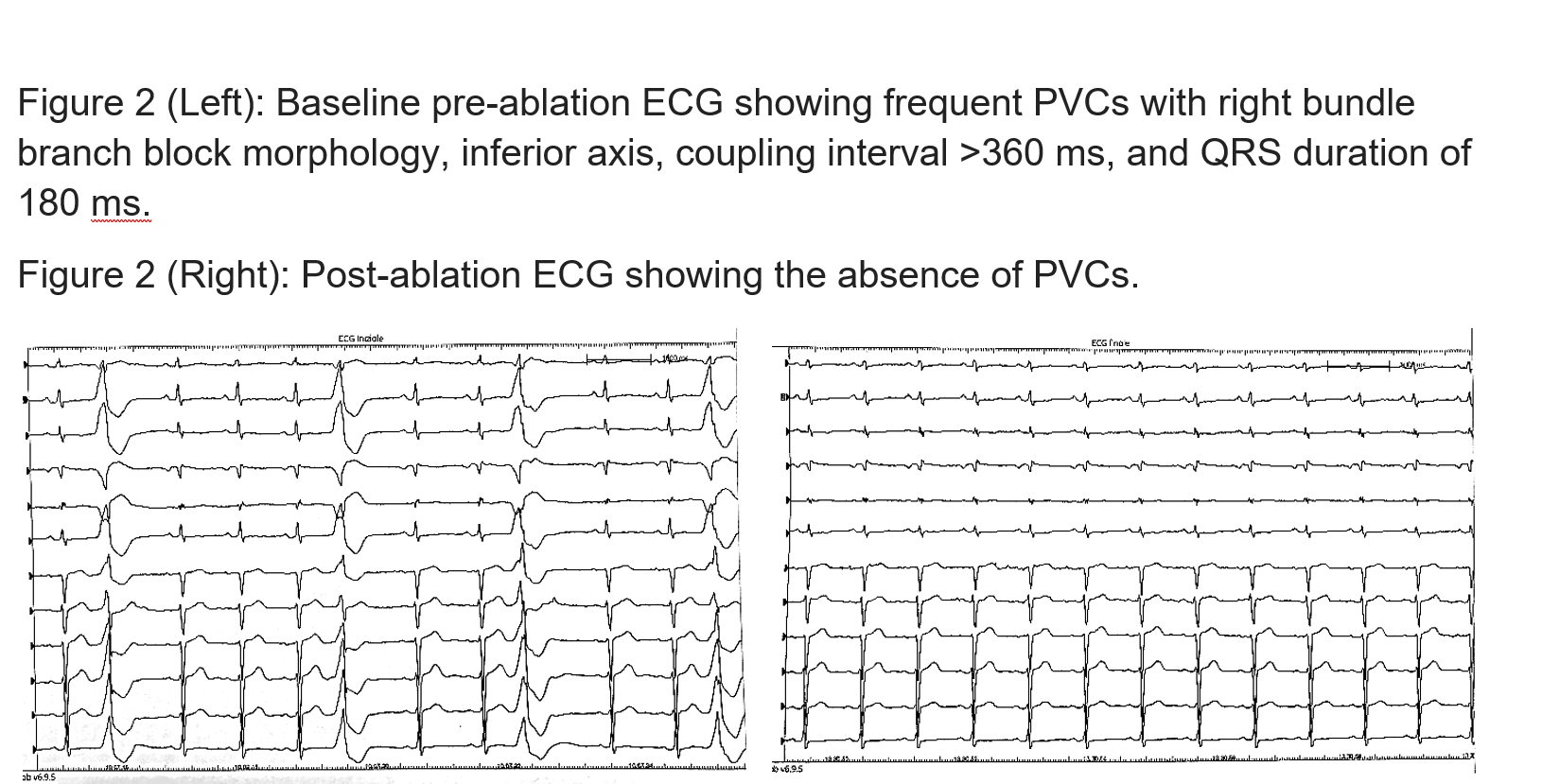
Introduction Premature ventricular contractions (PVCs) are frequently benign. However, a high arrhythmic burden can lead to the deterioration of left ventricular systolic function, resulting in newly developed cardiomyopathy or worsening of pre-existing cardiopathy. 2022 ESC guidelines for the management of ventricular arrhythmias recommend catheter ablation as class I treatment for patients with frequent PVCs and left ventricular dysfunction. Left ventricular summit is a muscular region surrounded by epicardial fat from which ventricular arrhythmias may originate. Case Report A 60-year-old man with known idiopathic dilated cardiomyopathy and moderate left ventricular dysfunction at cardiac magnetic resonance imaging (left ventricular ejection fraction 39%, areas of intramyocardial late enhancement) presented with worsening NYHA class. An echocardiogram documented deterioration of left ventricular systolic function (LVEF 25%), and a 24-hour Holter ECG revealed frequent monomorphic PVCs (approximately 20,000/24h) with right bundle branch block morphology, inferior axis, coupling interval >360 ms, and QRS duration of 180 ms. Catheter ablation of the arrhythmia was performed. An activation map of the left ventricle and subaortic region was constructed, using a THERMOCOOL SMARTTOUCH® (Biosense Webster) irrigated ablation catheter and the CARTO 3 mapping system. This revealed a wide anterolateral basal area with slightly anticipated electrograms relative to the QRS (-10 ms). Suspecting an epicardial origin of the PVCs from the left ventricular summit, an anterograde approach through the coronary sinus was attempted, identifying a significantly earlier ventricular signal (-48 ms) at the anterolateral left ventricle region. Coronary angiography excluded proximity to the circumflex coronary artery, and a single radiofrequency application resulted in PVC elimination, followed by additional consolidation lesions. At a six-month ambulatorial follow-up, the patient reported dyspnea regression, with echocardiographic LVEF improving to 37%. At three years post-ablation, LVEF had increased to 43%, with unchanged medical therapy. Discussion Catheter ablation of PVCs is the first-line treatment for patients with tachycardiomyopathy or worsening of known cardiomyopathy, considering the limitations of antiarrhythmic drugs. This case confirms the effectiveness of this approach in a patient with a high arrhythmic burden and primary dilated cardiomyopathy.