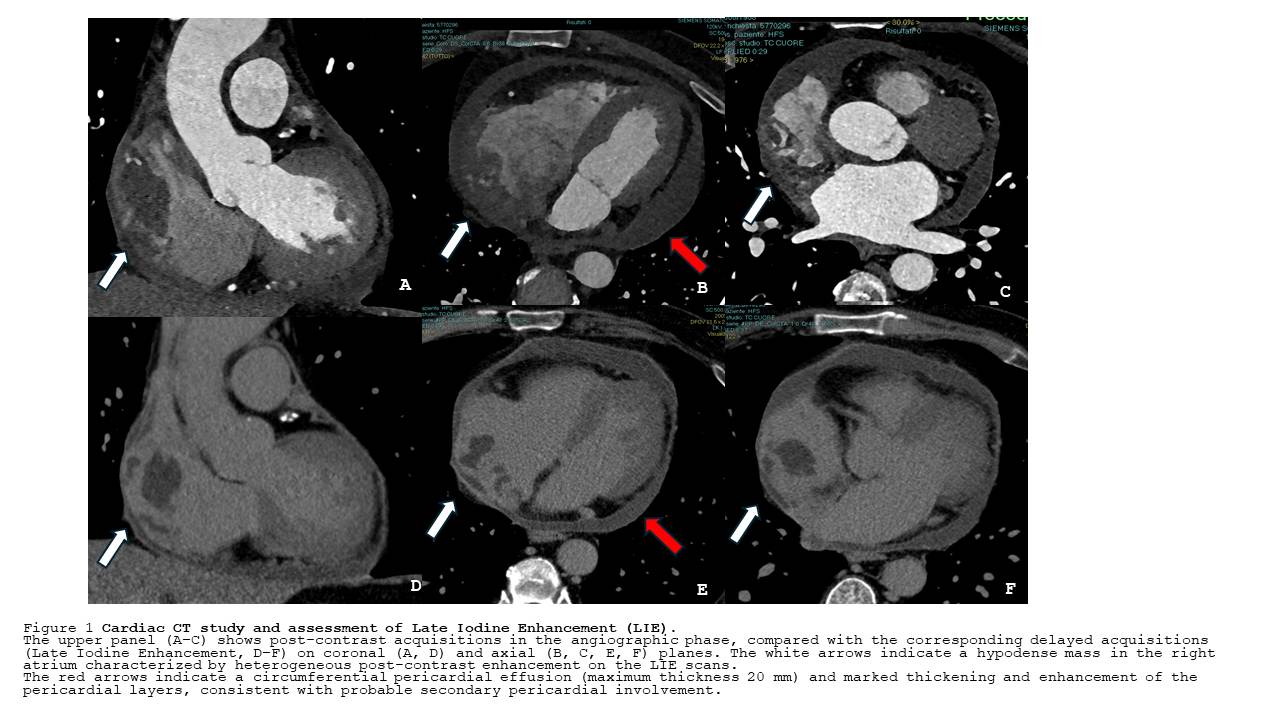
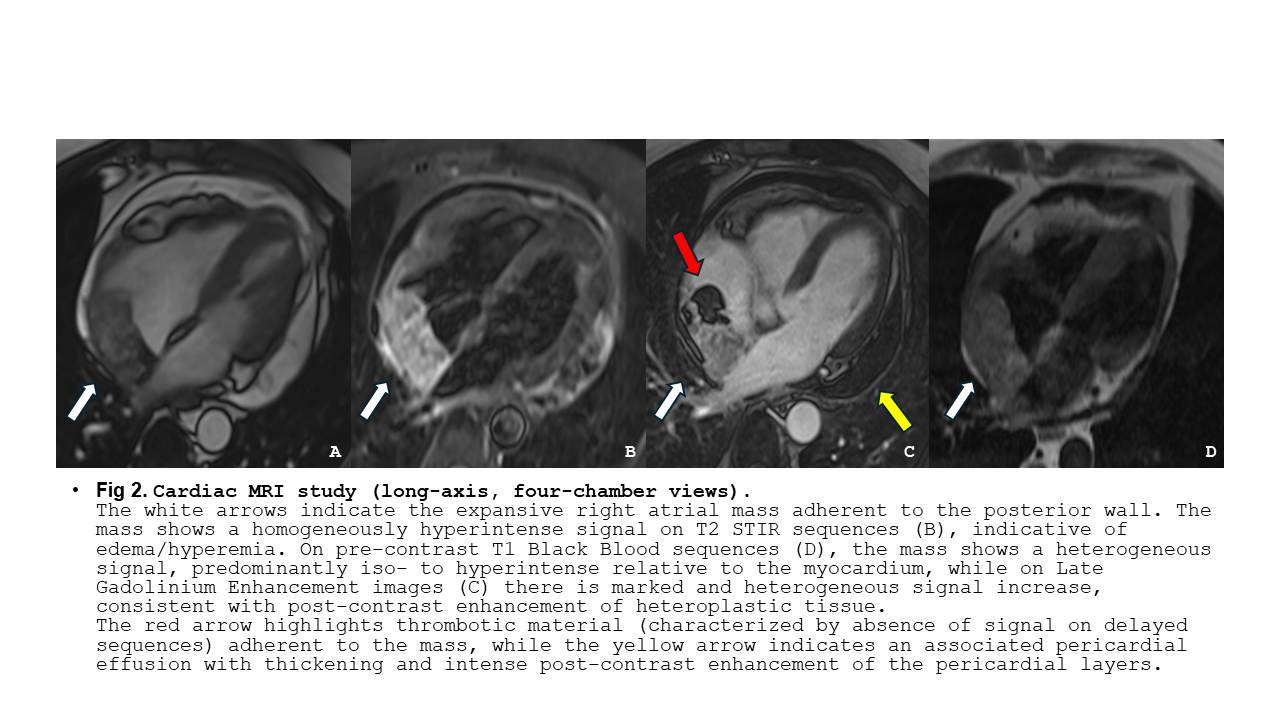
Atrial fibrillation (AF) is rarely the initial manifestation of an underlying cardiac malignancy and persistent pericardial effusion (PE) after AF ablation should prompt further investigation. A 67-year-old man underwent catheter ablation for symptomatic AF without complication or acute PE. 3 months later he developed fever and progressive dyspnea with elevated inflammatory markers. Echocardiography revealed a mild circumferential PE, confirmed by chest computed tomography (CT) which showed pulmonary micronodules too. Anti-inflammatory therapy with ibuprofen and colchicine was initiated. Fever persists and heart failure symptoms led to hospital admission. Repeat echocardiography revealed persistent PE and also a large echogenic mass arising from the roof of the right atrium and extending toward the superior vena cava, causing partial obstruction. Coronary CT confirmed the right atrial mass (RAM), associated pericarditis and multiple mediastinal lymphadenopathies(Fig.1). Cardiac magnetic resonance imaging demonstrated a heterogeneous RAM with features suggestive of a malignant cardiac tumor, without evidence of myocardial involvement(Fig.2). The patient was referred to a tertiary oncology center, where histological diagnosis confirmed primary cardiac angiosarcoma. Given the advanced stage of disease and extracardiac involvement, a multidisciplinary team opted for palliative oncological management. Discussion Late PE following AF ablation is an uncommon complication, usually related to a delayed inflammatory response and typically responsive to anti-inflammatory therapy. In this case the lack of clinical improvement and the unexpected finding of a RAM prompted further investigation. PE is a rare but recognized manifestation of primary cardiac angiosarcoma. This malignancy predominantly affects males and typically arises in the right atrium, with invasion of adjacent structures. Cardiac angiosarcoma is characterized by aggressive growth and early metastatic spread (commonly the lungs) resulting in a poor prognosis. Diagnosis relies on multimodality imaging while histological confirmation remains essential. Treatment strategies are not standardized and often involve palliative chemotherapy or surgical debulking. This case underscores the importance of maintaining a high index of suspicion for alternative diagnoses when PE persists or progresses after AF ablation. Early use of multimodality imaging is crucial for timely diagnosis and appropriate management.