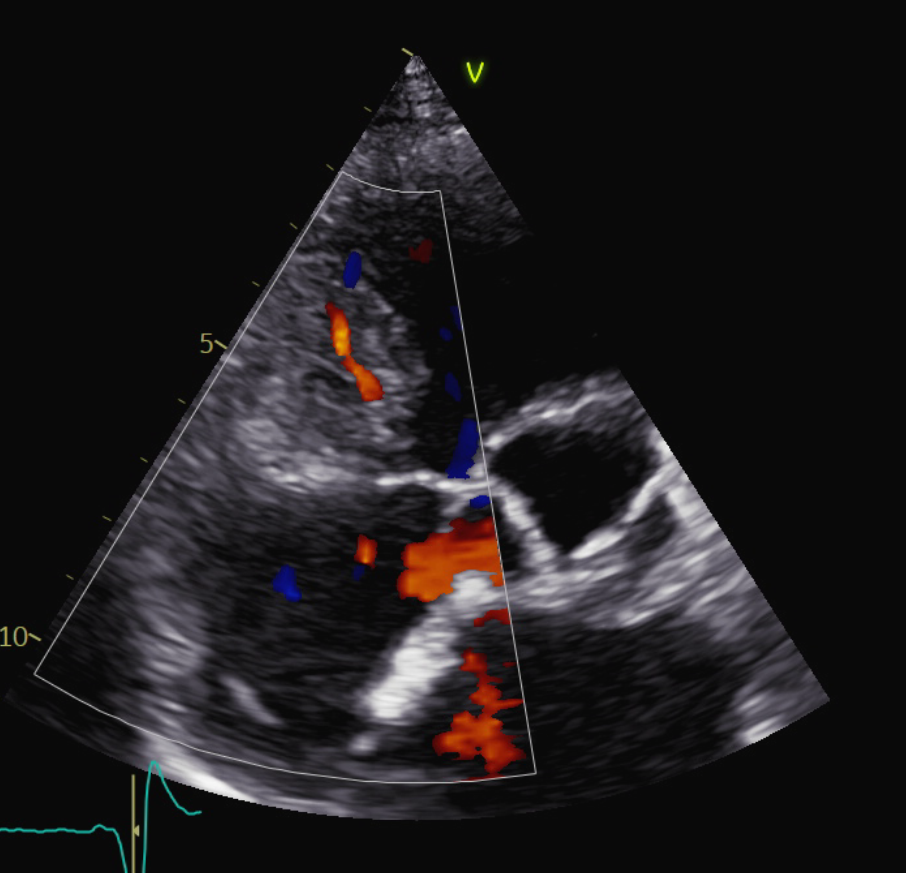
Case presentation: An 54-year-old woman with pacemaker implanted for sinus node dysfunction was asymptomatic at routine follow-up. Transthoracic echocardiography revealed a well-circumscribed, oval formation (35–38 mm) located anterior to the right ventricular (RV) inflow at the atrioventricular junction, causing mild extrinsic impression on RV without diastolic obstruction. Transesophageal echocardiography (TEE) was performed for better assessment. TEE showed a lesion with an internal echogenic rim consistent with stratified mural thrombosis and a central anechoic fluid component. Color Doppler identified a small intralesional vessel with low-velocity systo-diastolic flow. Agitated‑saline contrast fully opacified right chambers without filling of the lesion, excluding communication with right cavities. Conversely, after SonoVue administration, the lesion demonstrated delayed filling occurring after opacification of right- and left-sided chambers, strongly suggesting an arterial blood supply . These echocardiographic findings suggested a coronary aneyrysm or pseudoaneurysm. Coronary CT angiography (CTA) confirmed a structure in the AV junction with partially thrombosed cavity, no communication with RV and a close relationship with the right coronary artery (RCA). Invasive coronary angiography showed no significant coronary stenoses and opacification of the pseudoaneurysmal cavity through a small orifice arising from the mid RCA. Discussion: Masses located anterior to the right-sided cardiac chambers represent a diagnostic challenge, as cystic lesions, extracardiac tumors, and vascular abnormalities may present with overlapping echocardiographic appearances. This case highlights how contrast echocardiography together with multimodality imaging is crucial for the diagnosis. Coronary pseudoaneurysms are uncommon, usually acquired (most often after percutaneous coronary intervention or cardiac surgery), and represent a contained rupture lacking normal arterial wall layers. They may be incidental or present with chest pain, ischemia, embolization, arrhythmias, or rarely rupture/tamponade. Diagnosis relies on multimodal imaging (CTA for anatomy/thrombus/relationships; angiography for the neck/feeder and possible endovascular therapy). Management is individualized and includes conservative surveillance for stable lesions, covered stents or coil/plug embolization, and surgery for large/expanding, symptomatic, infected, or high‑risk anatomy.