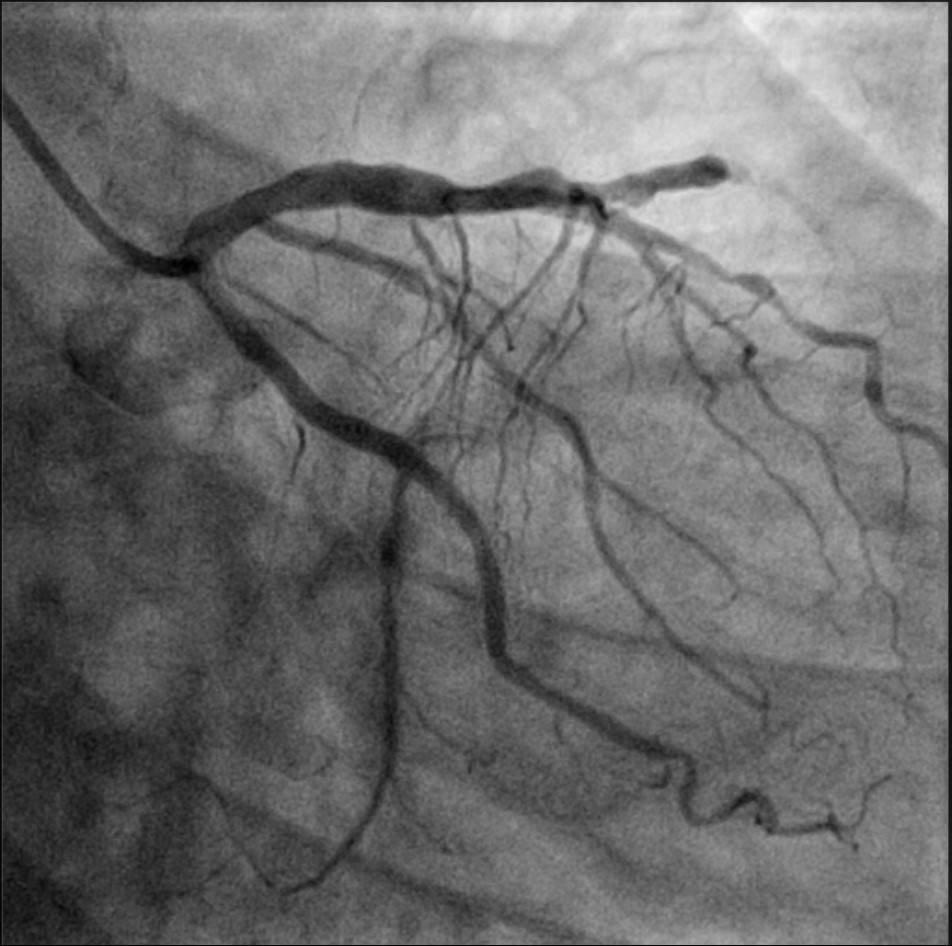
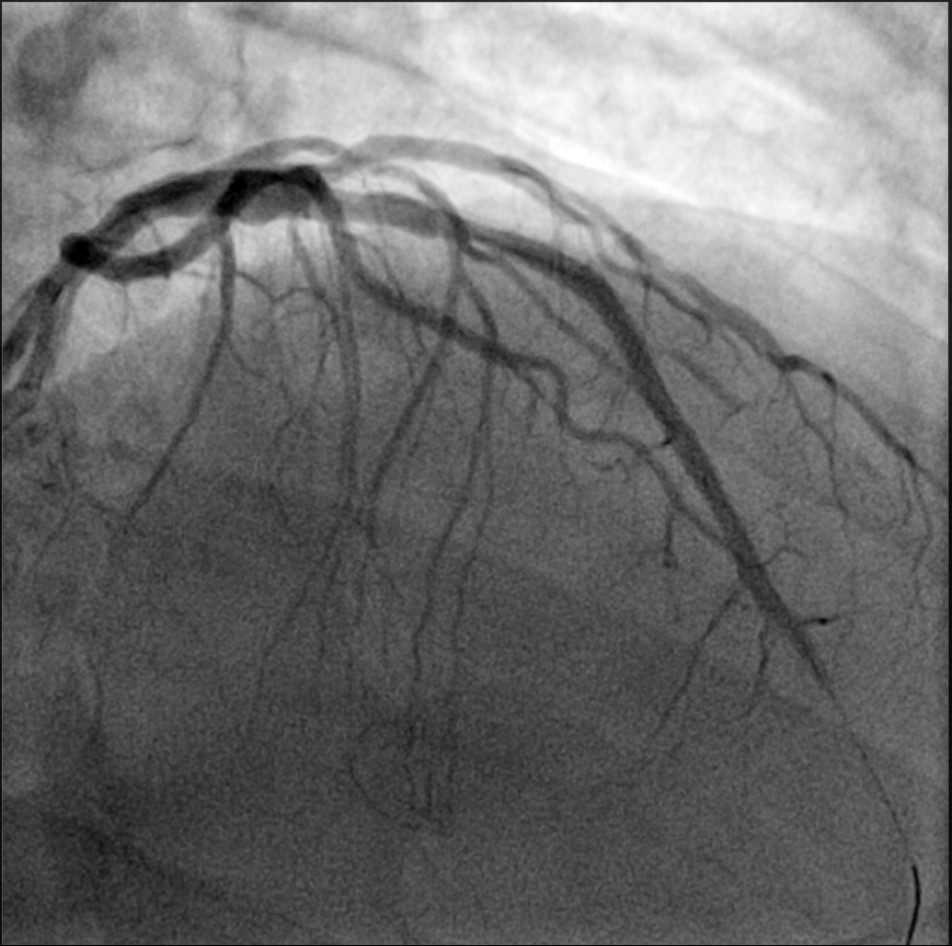
A 71-year-old man presented to the emergency department with a sensation of retrosternal heaviness that had begun several hours earlier. His medical history included arterial hypertension and previous smoking, and he was on antihypertensive therapy at home. He also reported experiencing similar symptoms when climbing stairs, which spontaneously resolved at the end of exertion. Laboratory tests were within normal limits, except for a slightly elevated high-sensitivity troponin level. Electrocardiogram: sinus rhythm with a heart rate of 60 beats per minute, normal atrioventricular and intraventricular conduction; no Q waves; minimal ST-segment elevation from V1 to V4 and slight ST-segment depression in leads I and aVL; wide-based T waves in V2-V3. The described findings did not meet the criteria for acute coronary syndrome with ST-segment elevation (STEMI) but were compatible with Occlusion Myocardial Infarction (OMI) of the left anterior descending (LAD) artery. The patient underwent transthoracic echocardiography, which revealed a non-dilated left ventricle with apical and mid-apical interventricular septum akinesia and a global ejection fraction of approximately 45%; no severe valvular disease was noted. The cardiac catheterization laboratory was promptly activated. Coronary angiography revealed an acute thrombotic occlusion of the mid-LAD segment, with the remainder of the epicardial coronary circulation free of significant lesions. Thromboaspiration was performed, followed by pre-dilation and deployment of a single drug-eluting stent at the culprit lesion. A no-reflow phenomenon occurred, necessitating optimized medical therapy and an infusion of glycoprotein IIb/IIIa inhibitors. The patient is currently stable and asymptomatic. Although the electrocardiographic findings did not meet the criteria for STEMI, they fulfilled the criteria for LAD OMI. The patient was therefore managed with immediate coronary angiography, allowing for early vessel recanalization compared to NSTEMI protocols, thereby reducing ischemic time. This case highlights the utility, as proposed in recent years, of transitioning from the STEMI-NSTEMI dichotomy to the OMI-NOMI paradigm.