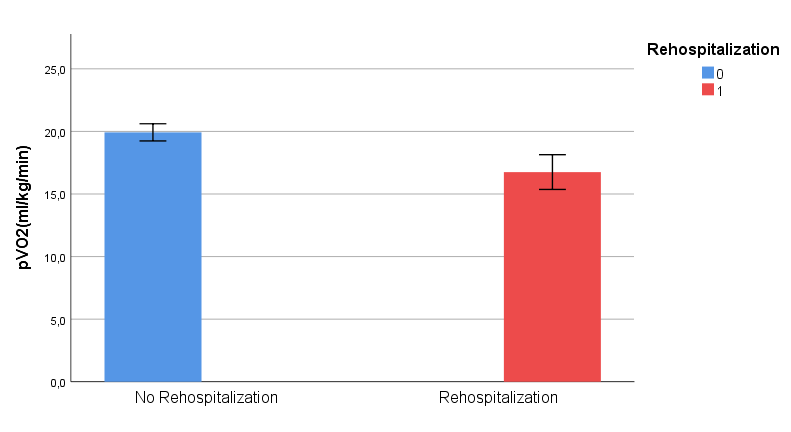
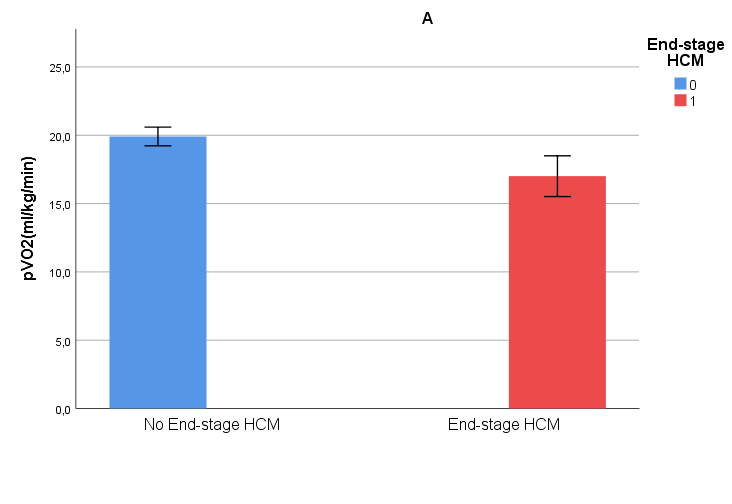
Introduction Hypertrophic cardiomyopathy (HCM) is a genetically driven myocardial disorder characterized by significant variability in clinical presentation and functional capacity (measured by peak oxygen consumption, pVO2). This study investigates the relationship between functional capacity and adverse events, focusing on rehospitalizations and progression to end-stage HCM. Methods 413 HCM p atients(46% obstructive; 63% male;mean age 48 years) were evaluated with CPET combined with concomitant transthoracic stress echocardiography at the cardiomyopathy unit of San Camillo Forlanini Hospital (Rome) Clinical outcomes included sudden cardiac death (SCD), progression to end-stage HCM, rehospitalization, myectomy, and implantable cardioverter-defibrillator (ICD) implantation. Results The mean pVO₂ for the cohort was 19.5 ml/kg/min, with 16% of patients demonstrating values below 50% of predicted levels. The mean pVO₂% was 68%, and the mean VE/VCO2 slope was 27. Echocardiographic findings showed an average ejection fraction (EF) of 66%, maximal left ventricular wall thickness of 20.5 mm, and peak LVOT gradients of 46 mmHg. Pulmonary artery systolic pressure was 20 mmHg at rest, rising to 36 mmHg during exercise. Mean filling pressure was higher than normal range (mean E/e’septal13.6; lateral: 9.2). During a mean follow-up of 8.7 years, 2.4% of patients progressed to end-stage HCM, and 8.2% underwent invasive interventions (e.g. myectomy or alcohol septal ablation). Device-based therapies (e.g. ICDs) were utilized in 8.2%, and aborted sudden cardiac death was reported in 0.7%. Disease progression to advanced NYHA classes occurred in 18.5% of patients, while rehospitalization in 10.7%. Rehospitalized patients exhibited significantly lower pVO₂ values (16.7 vs 19.9 ml/kg/min, pVO₂% 62 vs 68%, p < 0.05), higher VE/VCO2 slopes (29 vs 27, p < 0.05), higher filling pressures (E/e’ 17.5 vs 13.2 p < 0.05), compared to those without rehospitalizations. Similarly, patients progressing to end-stage HCM (11.1%) showed reduced functional capacity (pVO₂ 17.0 vs 19.9 ml/kg/min, pVO₂% 58.8 vs 78%, p<0.05), higher filling pressures (E/e’ 17 vs 13, p < 0.05), compared to the others Conclusions This study highlights the pivotal role of reduced functional capacity in predicting adverse outcomes in HCM. Patients with lower pVO2 are at significantly higher risk of rehospitalizations and progression to end-stage disease, spotting the light on this important clinical information