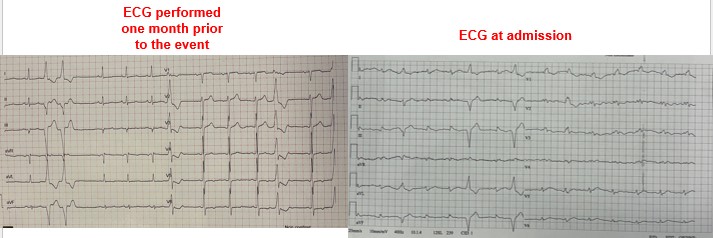
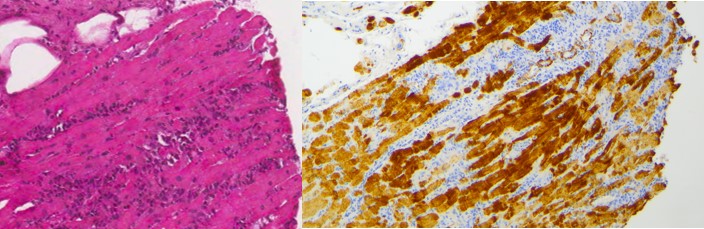
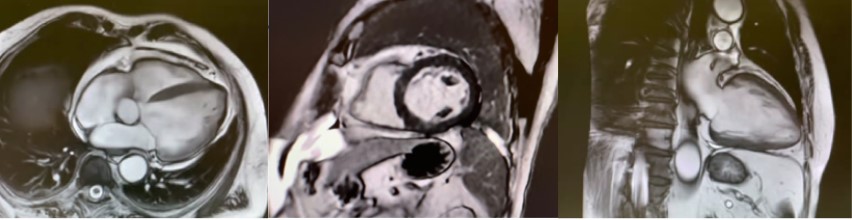
We report the case of a 67-year-old male who presented to a spoke emergency department with marked asthenia and dyspnea following an episode of acute gastroenteritis. Upon triage, the patient was assigned a red code due to hypotension and signs of hypoperfusion. Initial arterial blood gas analysis revealed metabolic acidosis with lactate levels of 2.7 mmol/L. Cardiological evaluation identified new-onset atrial fibrillation and severe left ventricular dysfunction (EF 10-15%) in the absence of ECG alterations suggestive of acute ischemia. Laboratory tests indicated multiorgan failure, with elevated creatinine and troponin levels. Based on these findings, dobutamine infusion was initiated, and the patient was subsequently transferred to a tertiary care center. Within hours, the patient experienced further hemodynamic deterioration, with lactate levels rising to 8 mmol/L, requiring escalation of inotropic support. Low QRS voltage on electrocardiogram compared to a prior tracing raised suspicion of myocarditis, prompting the administration of high-dose methylprednisolone therapy. Despite these measures, the clinical course rapidly progressed necessitating the implantation of IABP and endotracheal intubation. Coronary angiography excluded significant coronary artery disease, while urgent endomyocardial biopsy revealed massive acute necrotizing myocarditis, predominantly lymphocytic. Based on these findings, immunosuppressive therapy with intravenous immunoglobulins was initiated in addition to inotropic support and corticosteroid therapy.Over the following days, the patient demonstrated gradual hemodynamic stabilization, lactate clearance, and partial recovery of ventricular function, preceded by a progressive increase in QRS voltage on ECG. By day 18, the patient exhibited significant improvement, with left ventricular ejection fraction increasing to 30-35% and normalization of most laboratory parameters. Cardiac magnetic resonance imaging revealed minimal late gadolinium enhancement, leading to the decision to delay ICD placement pending reevaluation at 3 months. Therefore, the patient was discharged to a cardiological rehabilitation structure. This case highlights the critical role of early mechanical and pharmacological support, alongside immunomodulatory therapy, in managing fulminant myocarditis. Notably, early electrocardiographic improvement preceded ventricular functional recovery, emphasizing the potential prognostic value of ECG changes.