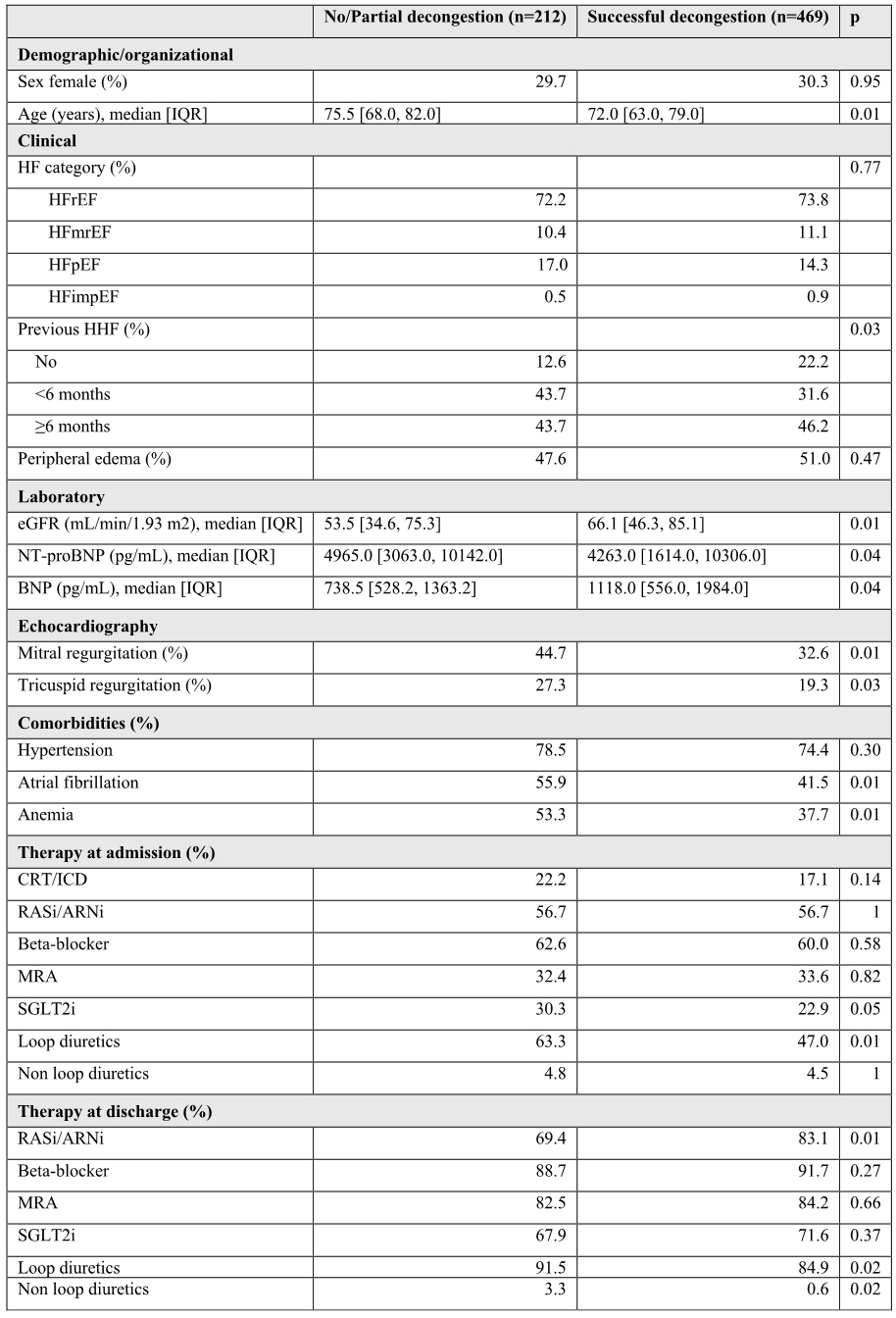
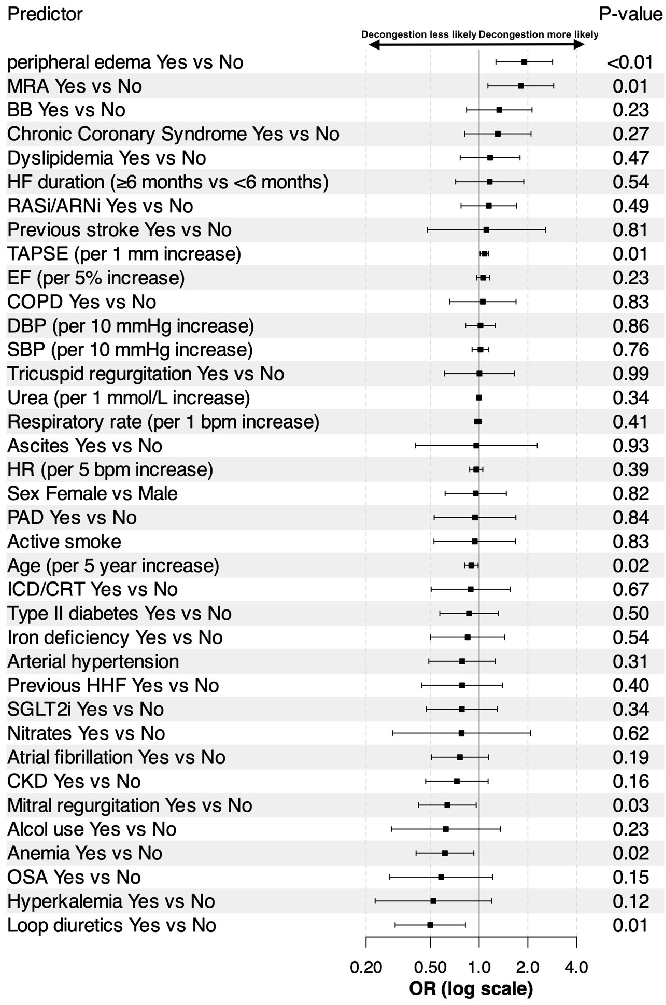
Introduction: Acute heart failure (AHF) is a critical condition requiring prompt intervention to alleviate fluid overload to reduce morbidity and mortality. However, there is still limited evidence on predictors of a successful decongestion at discharge. Purpose: To identify predictors of successful decongestion at discharge in patients hospitalized with AHF. Methods: The BRING-UP-3 HF study is an observational, prospective, multicenter observational study conducted across a large and representative sample of 179 Italian cardiology sites. For this analysis, we included patients hospitalized with AHF. We assessed predictors of successful decongestion at discharge, defined as the combination of clinical decongestion (≥1 kg weight loss or in NYHA class I/II at discharge) and biochemical decongestion (NT-proBNP at discharge <1500 pg/mL or BNP at discharge <250 pg/mL or ≥30% reduction in natriuretic peptides between admission and discharge), using multivariable logistic regression. Results: After excluding patients with missing data for natriuretic peptides, weight, and NYHA class, 681 patients (median age 73 years, 60% female) were included. Full decongestion was achieved in 469 (69%) patients. Factors significantly associated with full decongestion included younger age, higher estimated glomerular filtration rate and lower natriuretic peptide levels at admission, no history of AHF hospitalization, and absence of anemia, atrial fibrillation, or valve regurgitation. Patients with full decongestion were more likely to receive renin-angiotensin system inhibitors (RASi)/angiotensin receptor neprilysin inhibitors (ARNi) and less likely to be prescribed loop or non-loop diuretics at discharge (Figure 1). Key predictors of successful decongestion at discharge were younger age, presence of peripheral edema, absence of mitral valve regurgitation and anemia, higher tricuspid annular plane systolic excursion, and baseline use of mineralocorticoid receptor antagonists (Figure 2). Conclusion: In patients with AHF, full decongestion was achieved in approximately two-thirds of patients and was associated with specific clinical characteristics. Full decongestion was associated with a higher prescription of RASi/ARNi and a lower prescription of diuretics at discharge. Younger age, absence of mitral regurgitation, and no baseline loop diuretic use were significant predictors of successful decongestion.