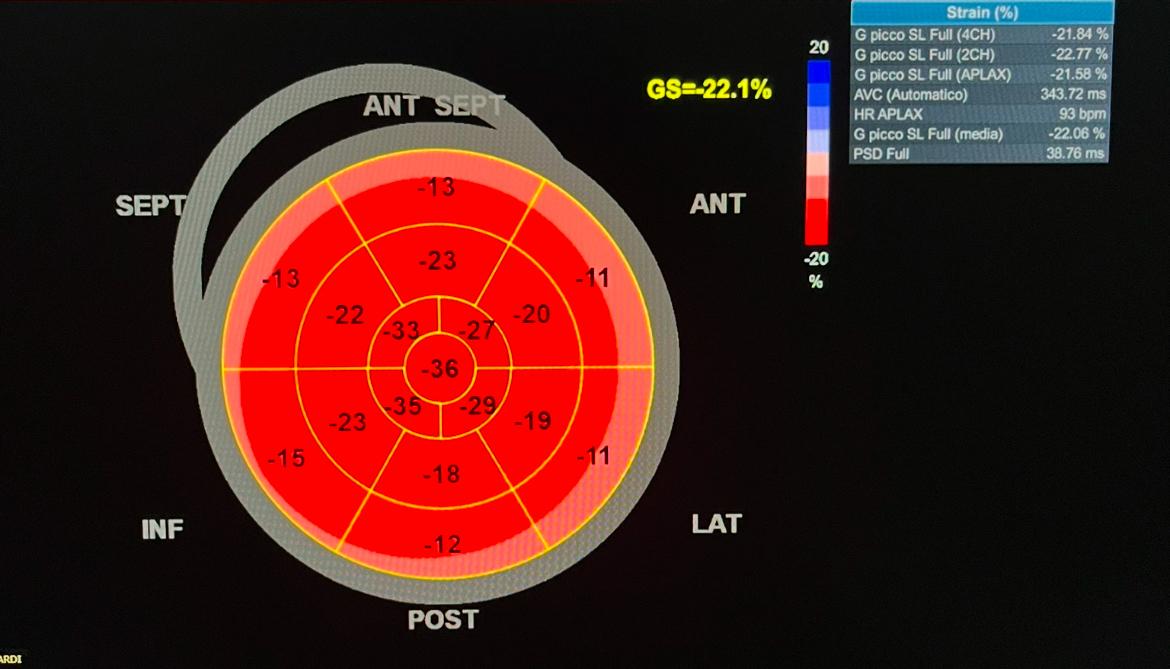
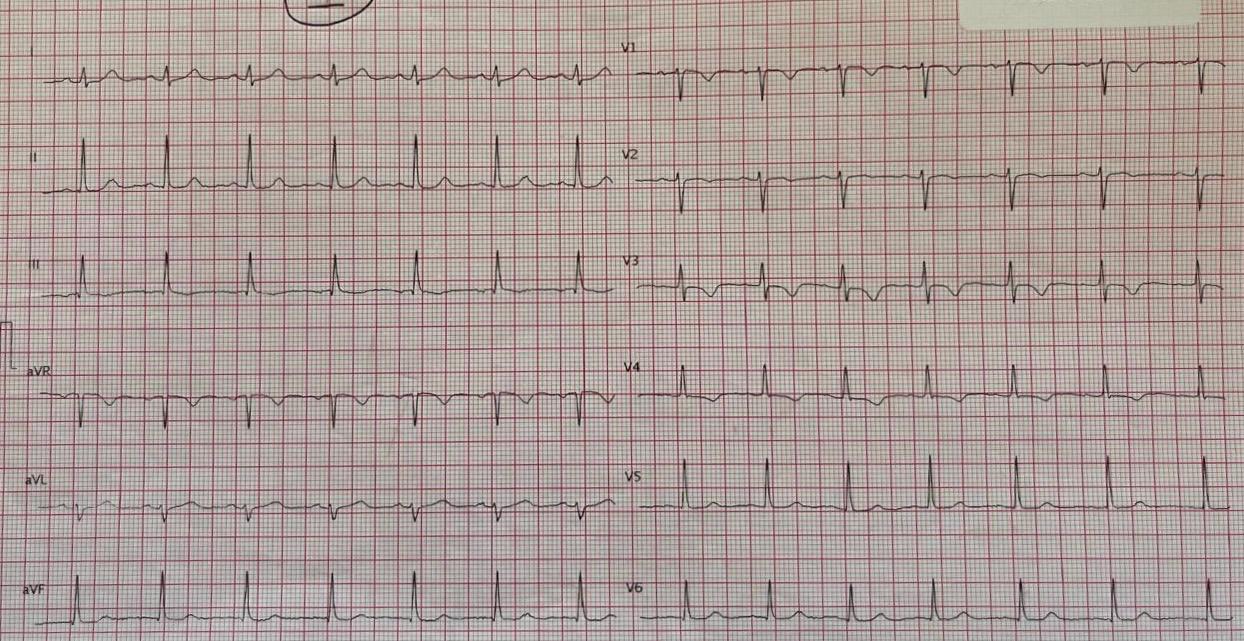
Case report: A 21-year-old female patient was admitted to the Hospital with nausea and fatigue appeared immediately after a verbal and physical aggression. She reported a story of pediatric long QT and a family medical history of long QT syndrome. The electrocardiogram (ECG) recorded negative T waves from V1 to V4. The blood sample analysis revealed a slight rise in TNI (peak 0,7 ng/ml, range of normality 0 – 0.034). The patient was transferred to the Intensive Cardiac Care Unit, where a Transtoracic Echocardiogram (TTE) showed moderate systolic dysfunction with a left ventricular ejection fraction (LVEF) of 45%, hypercontractility of the apical segments and mid-basal segments akinesia associated with moderate functional mitral regurgitation. Global longitudinal strain was abnormally low at −22% and was mainly impaired in the basal segments. A cardiac magnetic resonance imaging (MRI) showed native T1 and T2 increased in relation to edema of the basal segments, confirming the diagnosis of Reverse Takotsubo. We observed a prolonged corrected QT interval at 499 ms and a mild hypokalemia, which was corrected. During the rest of hospitalization no rhythm disorder was recorded, cardiac biomarker levels decreased and we observed the normalization of the T waves. On the six day of the hospitalization, TTE revealed an improvement in basal wall contraction (LVEF 58%) and a reduction of mitral regurgitation. The patient left the hospital in good clinical condition with a scheduled follow-up visit. Take home message: Reverse Takotsubo syndrome (rTTS) is a variant of the Takotsubo syndrome (TTS) characterized by the basal akinesis/hypokinesis associated with apical hyperkinesis. The assocation between Congenital Long QT and TTS is rare and few cases are reported in the literature. The prevalent arrhythmic complication described was torsade de pointes. Diagnostic criteria of TTS include transient regional wall motion abnormalities, absence of angiographic evidence of obstructive coronary disease, presence of ECG abnormalities or troponin elevation and exclusion of pheochromocytoma or myocarditis. In this case the age of the patient, the topography of the wall motion abnormality and the MRI-results were not evocative of an ischemic process and we diagnosed a reverse TTS without using coronary angiography. Moreover, the echocardiographic follow-up of wall motion abnormalities, LVEF and strain pattern allowed us to confirm the rTTS by showing a full recovery.