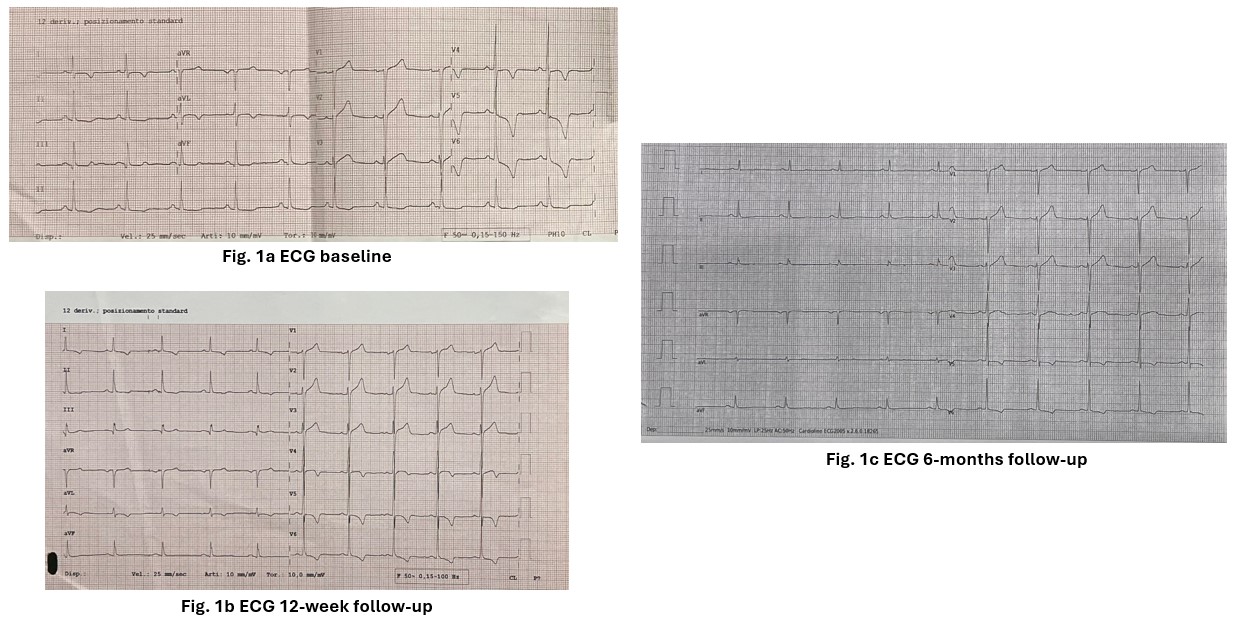
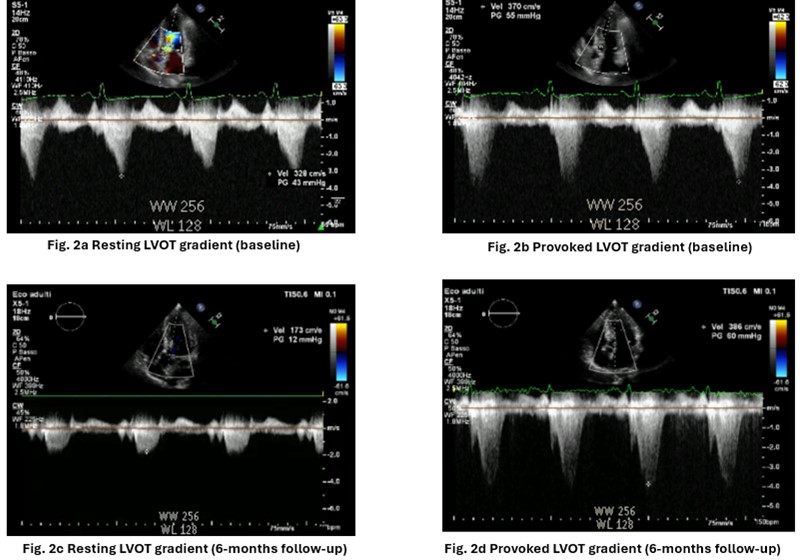
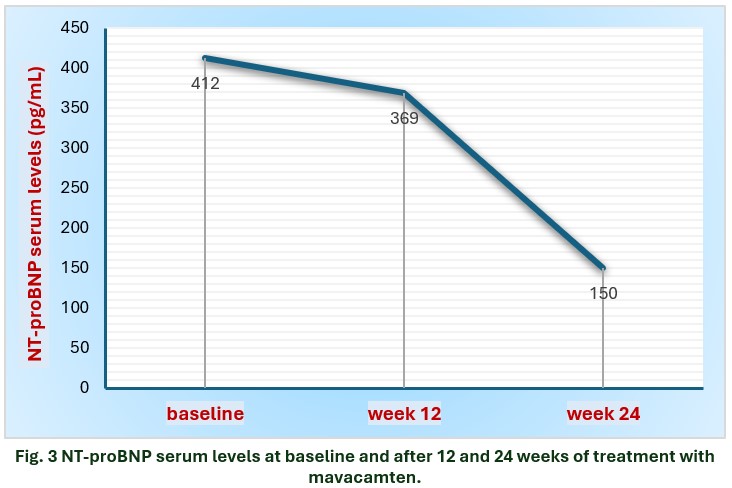
A 54-year-old male was diagnosed in 2018 with hypertrophic obstructive cardiomyopathy (HOCM); genetic test negative for Sarcomeric HCM mutations. No relevant comorbidities. Cardiac MRI revealed intramyocardial LGE in inferolateral, anterior and septal regions. He was receiving nadolol 80 mg once daily (o.d.) due to hemodynamically significant latent LVOT obstruction at transtoracic echocardiography (TTE). HCM risk score was 2.9%/5 years. In early 2024, during a follow-up (FU) visit at our CMP clinic, the patient reported moderate exertional dyspnea (NYHA II). EKG revealed sinus rhythm, signs of left ventricular hypertrophy, and marked repolarization abnormalities in the high lateral and lateral leads (Fig. 1a). TTE showed severe asymmetric HCM with septal hypertrophy (IVS 20 mm) and LVOT obstruction (peak gradient – PG – of 43 mmHg at rest and 55 mmHg during Valsalva) (Fig. 2a-2b). LVEF was 77%. Left atrium (LA) was dilated (69 mL/m²) with mild-to-moderate (baseline) to moderate-to-severe (Valsalva) mitral regurgitation (MR). Stress echocardiography (SE) confirmed the baseline TTE findings and also revealed latent grade II diastolic dysfunction. Genotyping for cytochrome P450 (CYP2C19) was performed to determine the correct individual starting dosage of Mavacamten. Then, compassionate use of mavacamten 5 mg (rapid metabolizer) was started. Baseline NT-proBNP was 412 pg/mL. 12-weeks (W) FU: symptoms improvement was noted. EKG showed a slight reduction in repolarization abnormalities (Fig. 1b) while TTE revealed a latent LVOT obstruction (PG of 55 mmHg). NT-proBNP was 369 pg/mL. 6-months FU: patient was on mavacamten 10 mg o.d., asymptomatic (NYHA I). EKG showed significant improvement with normalization of repolarization in the high lateral leads and V4, and a decrease in the voltage of negative T waves in V5-V6 (Fig. 1c). SE still revealed latent LVOT obstruction (PG of 60 mmHg), but improved diastolic function and reduced MR severity during exertion (Fig. 2c-2d). A marked decline of NT-proBNP serum levels (from 412 to 150 pg/mL; Fig. 3) and a reduction in IVS thickness and LA volume were observed. LVEF was > 55%, so mavacamten was up-titrated to 15 mg o.d., with a planning to reassess patient after 4 W. Conclusions: This clinical case suggests that mavacamten globally impacts on the pathophysiology of HCM (reduction of LVOT obstruction, mitral regurgitation, diastolic function) leading to dramatic improvements of ECG abnormalities and NT pro BNP levels.