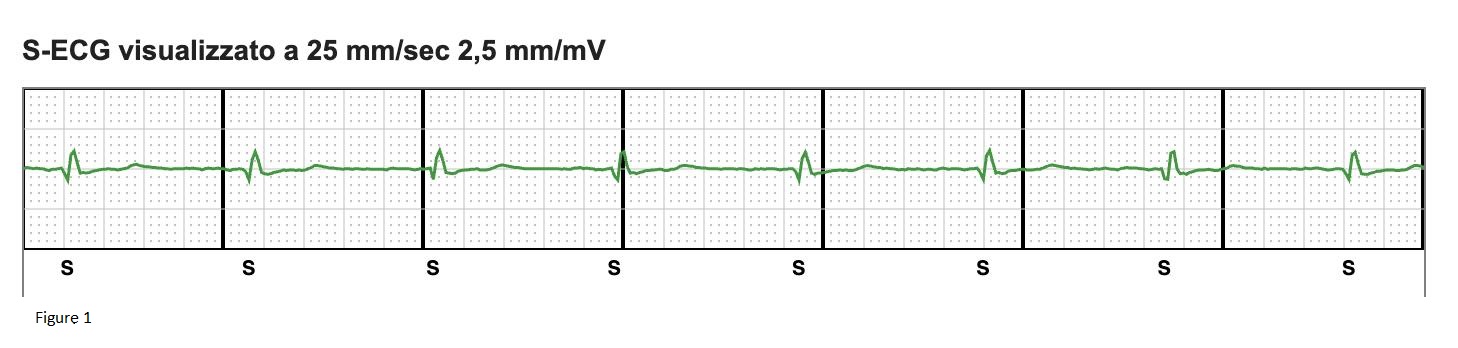
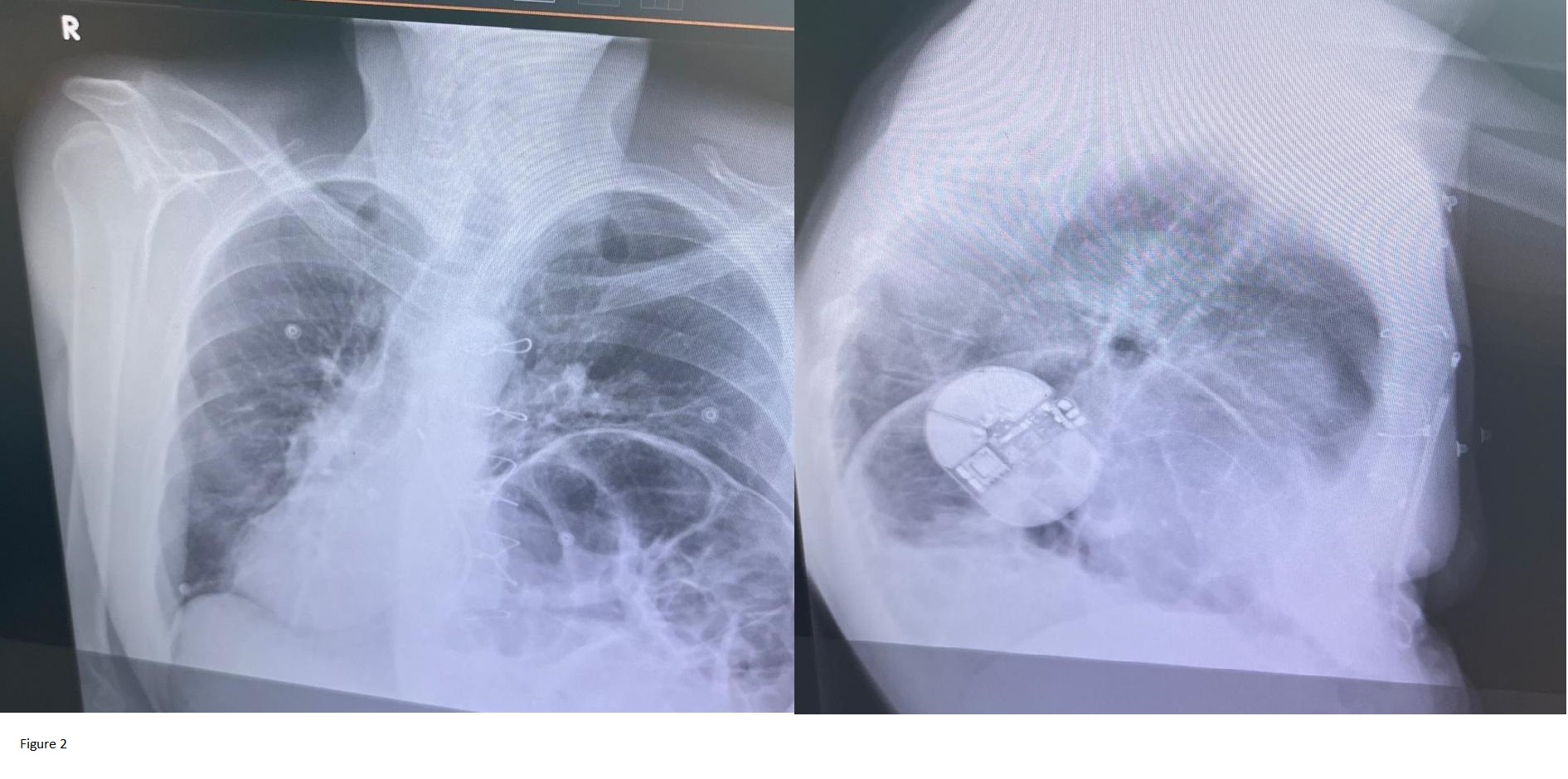
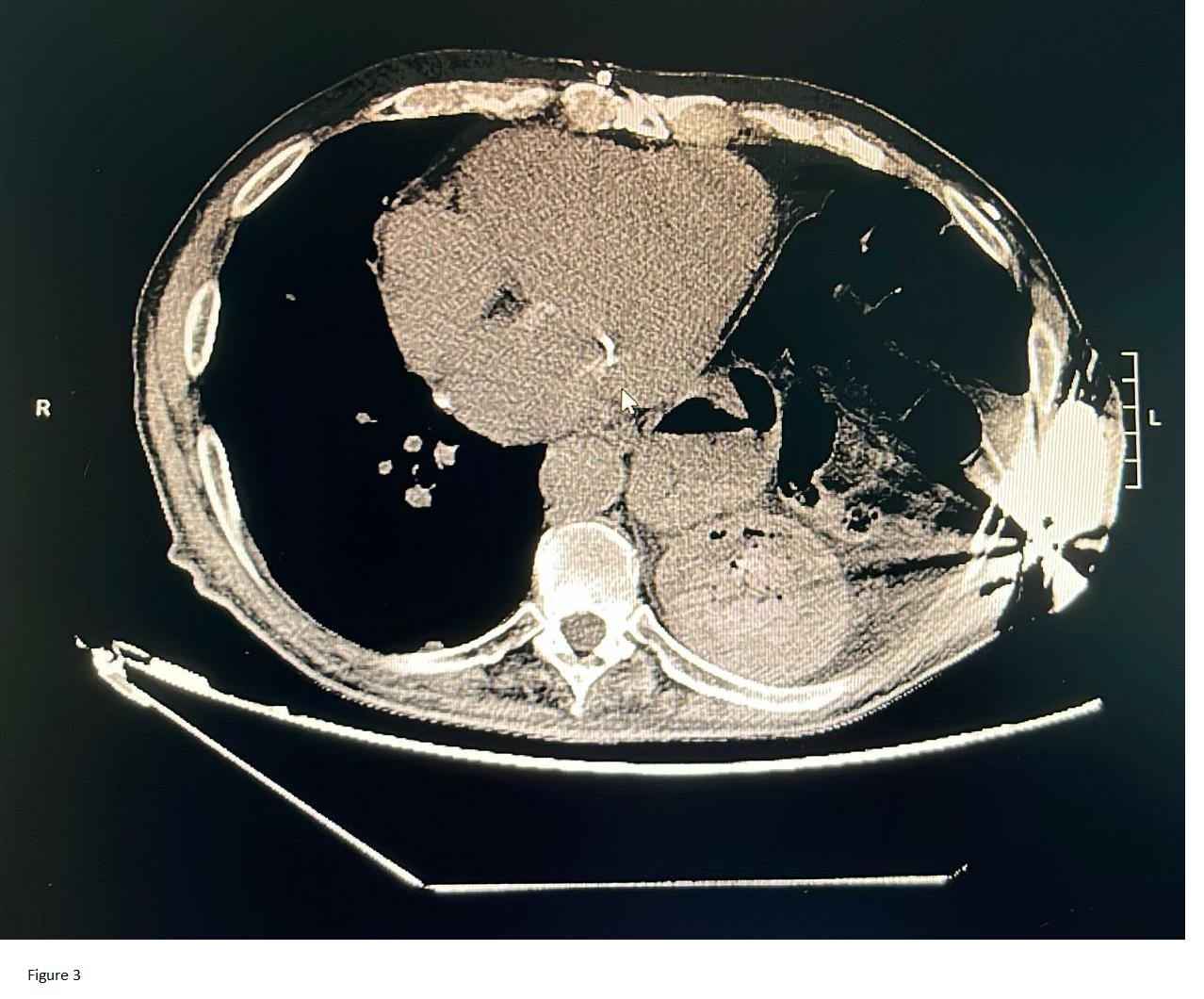
Background Growing evidence supports omitting defibrillation testing (DFT) during subcutaneous ICD (S-ICD) implantation. The PRAETORIAN score, based on two-view chest X-ray findings, accurately predicts defibrillation efficacy, allowing clinicians to avoid discomfort and risks associated with DFT. However, certain anatomical variations may limit its applicability. Case presentation We present the case of a 76-year-old male who underwent S-ICD implantation for primary prevention of sudden cardiac death. His history included severe left ventricular dysfunction due to chronic coronary syndrome, permanent atrial fibrillation, and two cardiac surgeries (mitral valve plastic with concomitant coronary artery bypass grafting and subsequent bioprosthetic mitral valve replacement). The second cardiac surgery was complicated by left phrenic nerve palsy and associated hemidiaphragm elevation. Pre-implantation fluoroscopy in the supine position confirmed the hemidiaphragm elevation and a slight rightward shift of the cardiac silhouette. The procedure was completed without complications, showing optimal S-ECG signals (Figure 1) and system impedance (55 ohm). Despite an optimal PRAETORIAN score (30 points), the post-implantation standing X-ray revealed a marked rightward mediastinal shift (Figure 2), suggesting the ventricular mass was almost entirely outside the defibrillation field and raising suspicion of high DFT failure risk. To better evaluate the three-dimensional (3D) relationship between the ventricular mass, the device can, and the lead, a chest CT scan was performed. The CT confirmed that the ventricular mass was appropriately contained within the defibrillation shock vector (Figure 3). Following consultation with technical support, we decided to omit DFT. The patient remains under remote monitoring with an uneventful follow-up. Conclusions Although the PRAETORIAN score is a reliable tool, specific anatomical conditions like phrenic nerve palsy can complicate radiological assessment. Image acquisition in the standing position and during deep inspiration may alter anatomical relationships, potentially leading to discrepancies between standard orthogonal views and the actual 3D shock vector. In such cases, a 3D CT evaluation can provide crucial clarification of the anatomical relationships between the device and the heart, potentially supporting the safe omission of DFT even when standard X-rays appear ambiguous.