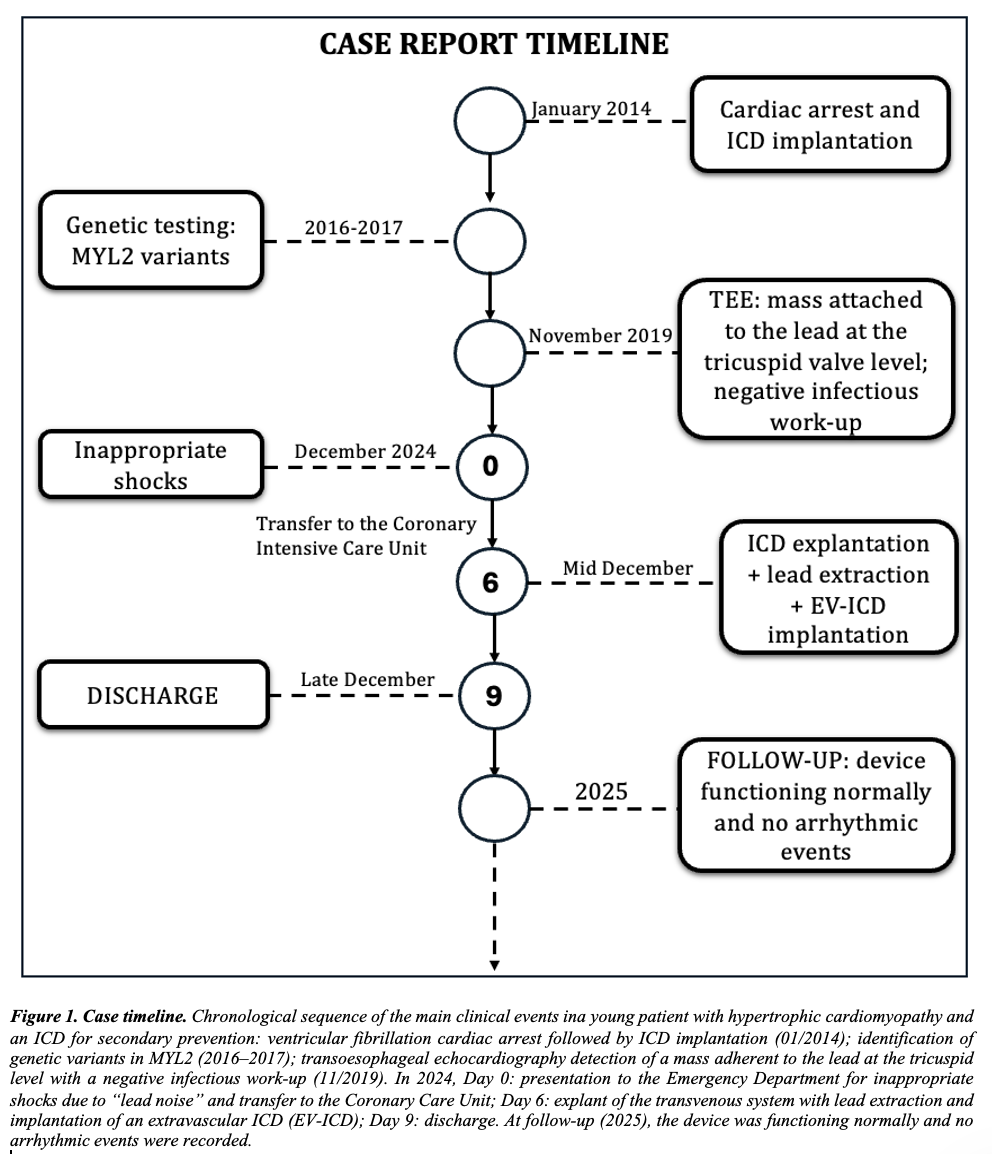
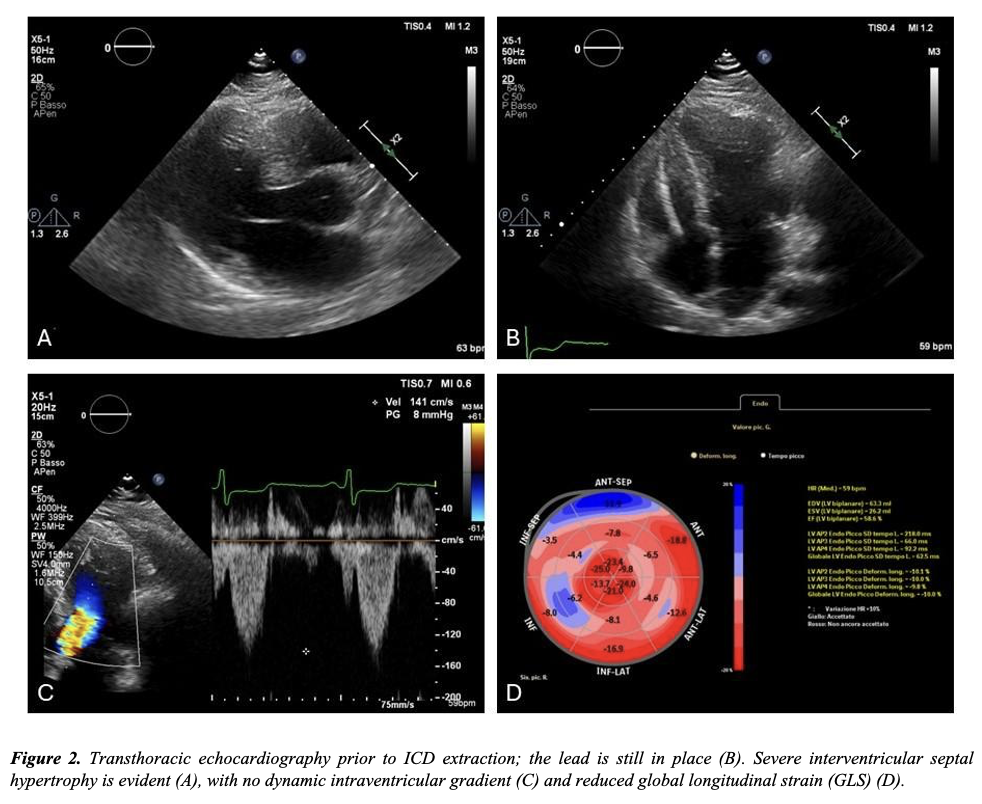
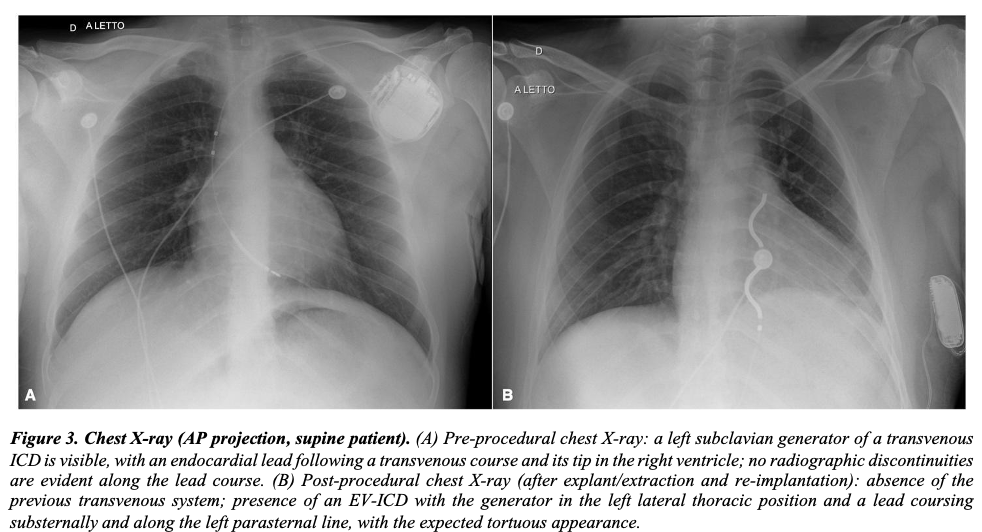
BACKGROUND: In hypertrophic cardiomyopathy (HCM), an implantable cardioverter-defibrillator (ICD) is a Class I recommendation according to ESC guidelines after resuscitated ventricular fibrillation. In young patients, however, decades of exposure to transvenous leads translate into a meaningful risk of lead failure, venous obstruction and infections. Subcutaneous ICDs avoid the vascular system and cardiac chambers but still cannot deliver antitachycardia pacing (ATP). The extravascular ICD (EV-ICD) places the lead in the substernal space, aiming to combine vascular sparing with ATP. CASE PRESENTATION: A 25-year-old man with HCM suffered an exercise-related cardiac arrest in 2014 (documented VF) and received a single-chamber transvenous ICD for secondary prevention. He presented with shocks occurring during sleep. Device interrogation showed five inappropriate shocks due to intermittent ventricular lead noise, and an elective replacement indicator (likely triggered by the shocks), while sensing and impedance were otherwise within range.Echocardiography confirmed severe septal hypertrophy (up to 28 mm), preserved ejection fraction (58%) with reduced global longitudinal strain (−10.9%), chordal systolic anterior motion and no significant intraventricular pressure gradient. A previously reported mobile mass adherent to the lead at the tricuspid annulus had remained clinically silent with a negative infectious work-up. Given recurrent inappropriate therapies, young age and the desire to limit long-term endovascular burden, the transvenous system was removed and the lead extracted. An EV-ICD (Aurora, Medtronic) was then implanted with a substernal lead and a left lateral generator pocket. Induced VF was promptly detected and terminated with a 30-J shock. The patient was discharged three days later and remained event-free with normal device function at early and mid-term follow-up. CONCLUSIONS: In selected young patients with strong ICD indications and transvenous lead complications, EV-ICD can represent a pragmatic compromise, reducing intravascular hardware while preserving defibrillation efficacy and ATP capability