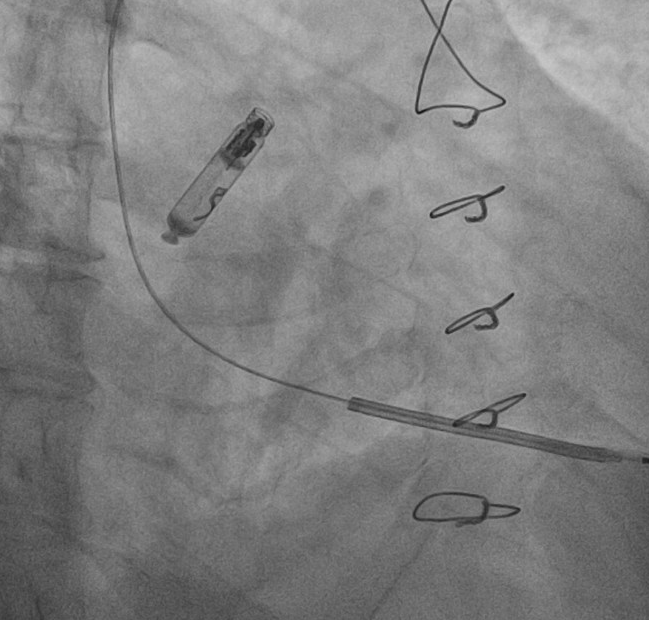
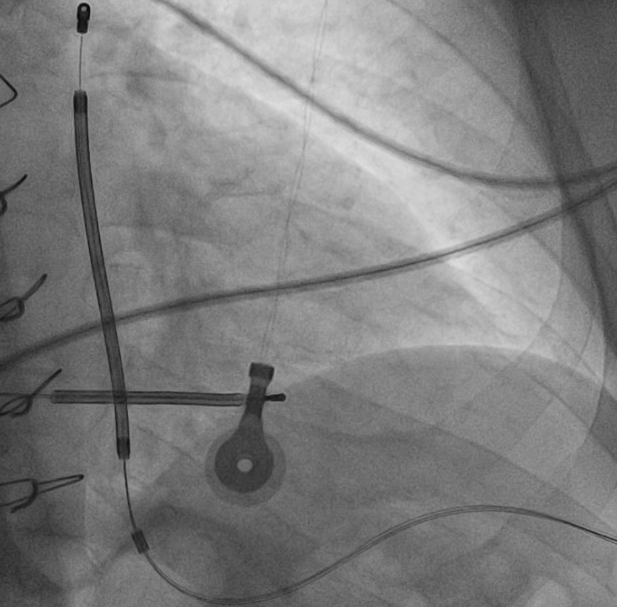
BACKGROUND: Managing patients who require both atrial pacing and sudden cardiac death (SCD) prevention is challenging, especially in young individuals who may face repeated device implantations. Combining a leadless atrial pacemaker with a subcutaneous defibrillator (S-ICD) can provide effective atrial pacing with preserved arrhythmic protection, minimizing infective and procedural risks inherent to transvenous systems. CLINICAL CASE: We present a 59-year-old man with hypertrophic obstructive cardiomyopathy (HOCM) and mitral valve disease. A single-chamber transvenous defibrillator (TV-ICD) was implanted in 2012 for primary prevention. In 2014, he underwent Morrow septal myectomy with mitral valve repair for severe regurgitation. Subsequently, he developed ischemic strokes in the setting of new-onset atrial fibrillation (AF). In 2023 transthoracic echocardiographic showed left ventricular hypertrophy with obstruction (gradient 80/39 mmHg), preserved function, systolic anterior motion with moderate MV regurgitation. In May 2025, device interrogation revealed ventricular pacing at 40 bpm (VVI 40 bpm) with underlying sinus rhythm at 38 bpm, first-degree atrioventricular block, and paroxysmal AF with ventricular rate up to 140 bpm, consistent with tachy-brady syndrome. Ventricular pacing burden was 12%. Defibrillation coil impedance was 120-130 Ohm. No ventricular arrhythmic episodes were registered on chronic amiodarone and beta-blocker therapy. Patient remained asymptomatic and clinically stable. After multidisciplinary discussion, a leadless atrial pacemaker was implanted in the right atrial appendage, followed one week later by an S-ICD, to provide atrial pacing and SCD prevention while avoiding the risks of repeated TV-ICD implantation. An implantable loop recorder was also implanted for continuous arrhythmic monitoring. CONCLUSION: This case highlights the feasibility and effectiveness of combining a leadless atrial pacemaker with an S-ICD in a complex HOCM patient with tachy-brady syndrome and high arrhythmic risk. This approach provides reliable atrial pacing and sudden cardiac death protection while minimizing infection and extraction risks associated with transvenous systems.