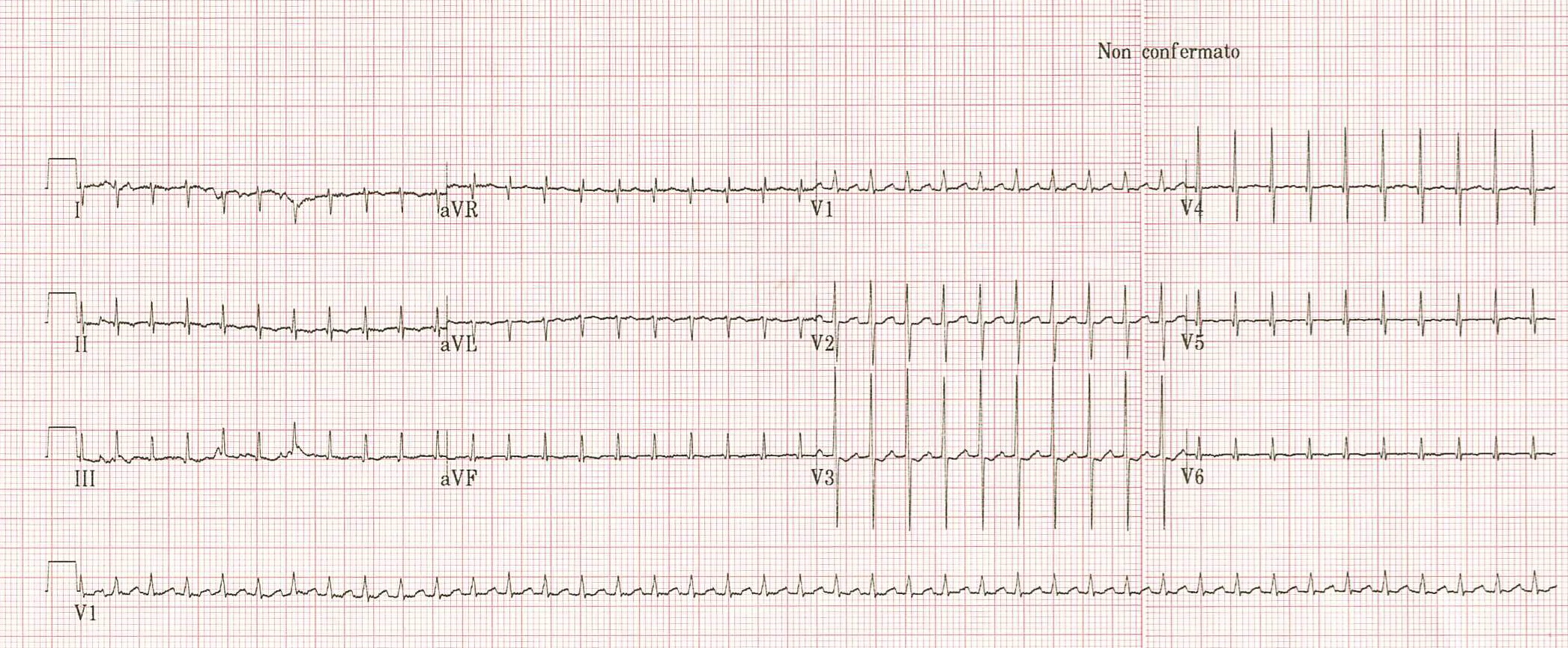
Background. Supraventricular tachycardia (SVT) is the most common neonatal arrhythmia. Rapid recognition and targeted therapy are essential to avert hemodynamic compromise and prevent tachycardia-induced cardiomyopathy. Case. A term female neonate (3.4 kg; Apgar 9/10) developed sustained narrow-complex tachycardia at 240 bpm within minutes of birth. Vagal maneuvers failed. Intravenous adenosine (0.2 mg/kg) abruptly restored sinus rhythm and unmasked a short PR interval (80 ms). Echocardiography and laboratory testing were unremarkable. During tertiary-center monitoring no recurrences occurred; prophylactic oral flecainide (2 mg/kg/day) was initiated. At two months, the infant remained asymptomatic with sinus rhythm (PR 98 ms). Interpretation. Immediate adenosine termination, coupled with a persistently short PR, strongly supports orthodromic atrioventricular re-entrant tachycardia via an accessory pathway (probable WPW physiology). In this age group, AVNRT is uncommon and does not explain marked PR shortening; atrial flutter typically shows saw-tooth activity and is seldom terminated by adenosine; focal atrial tachycardia usually displays warm-up/cool-down and rarely stops abruptly. Management and implications. Adenosine is both diagnostic and therapeutic in neonatal SVT, helping reveal concealed pre-excitation that informs risk stratification. Current pediatric practice favors inpatient observation after a first episode and selective prophylaxis; flecainide is effective for early-life recurrence prevention. Electrophysiological study/ablation is generally deferred unless drug-refractory recurrences, drug intolerance, or high-risk pre-excitation persists. Conclusion. This case underscores that prompt ECG-based diagnosis and adenosine-guided management enable safe early stabilization of neonatal accessory-pathway–mediated SVT, with excellent short-term outcomes.