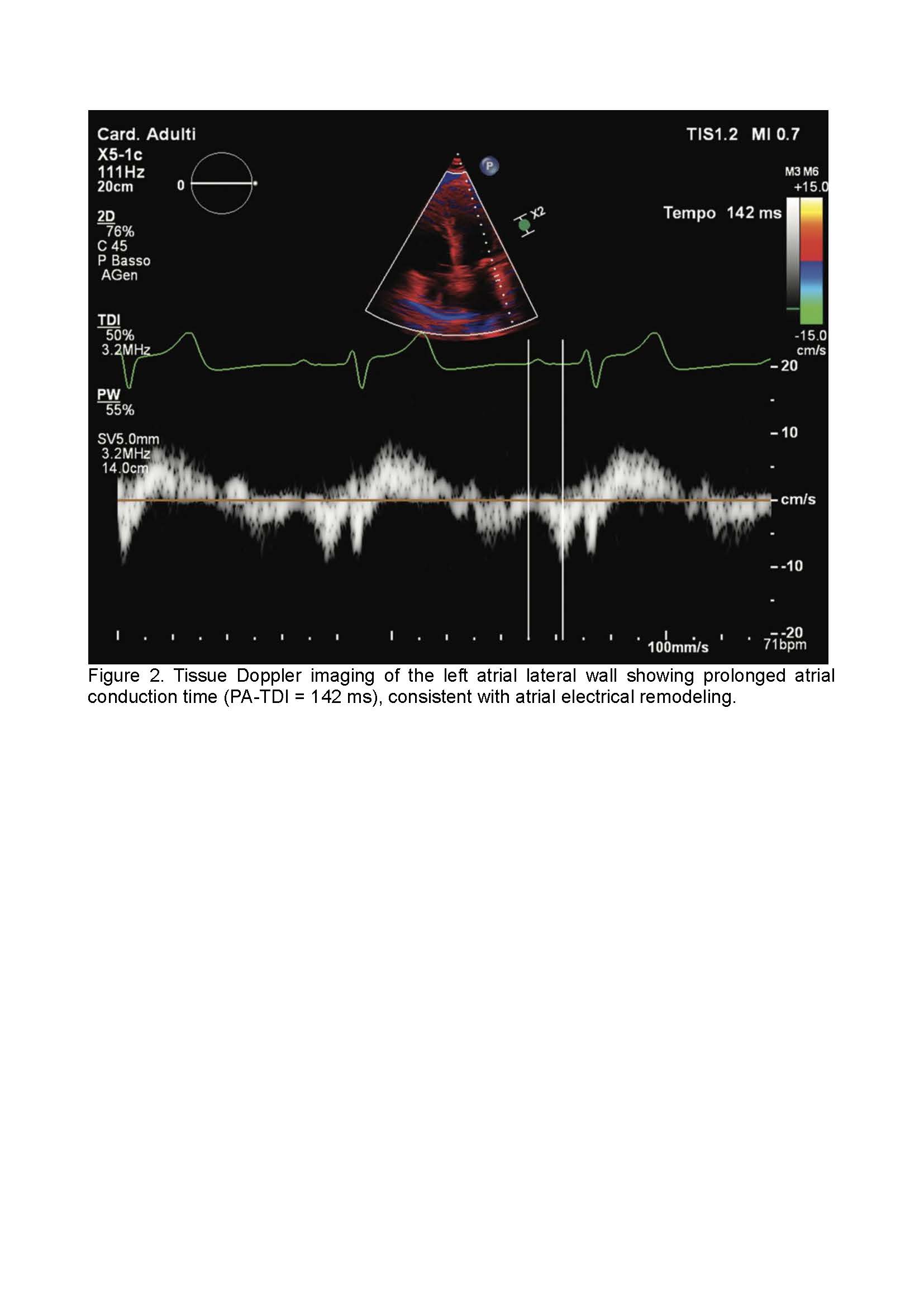
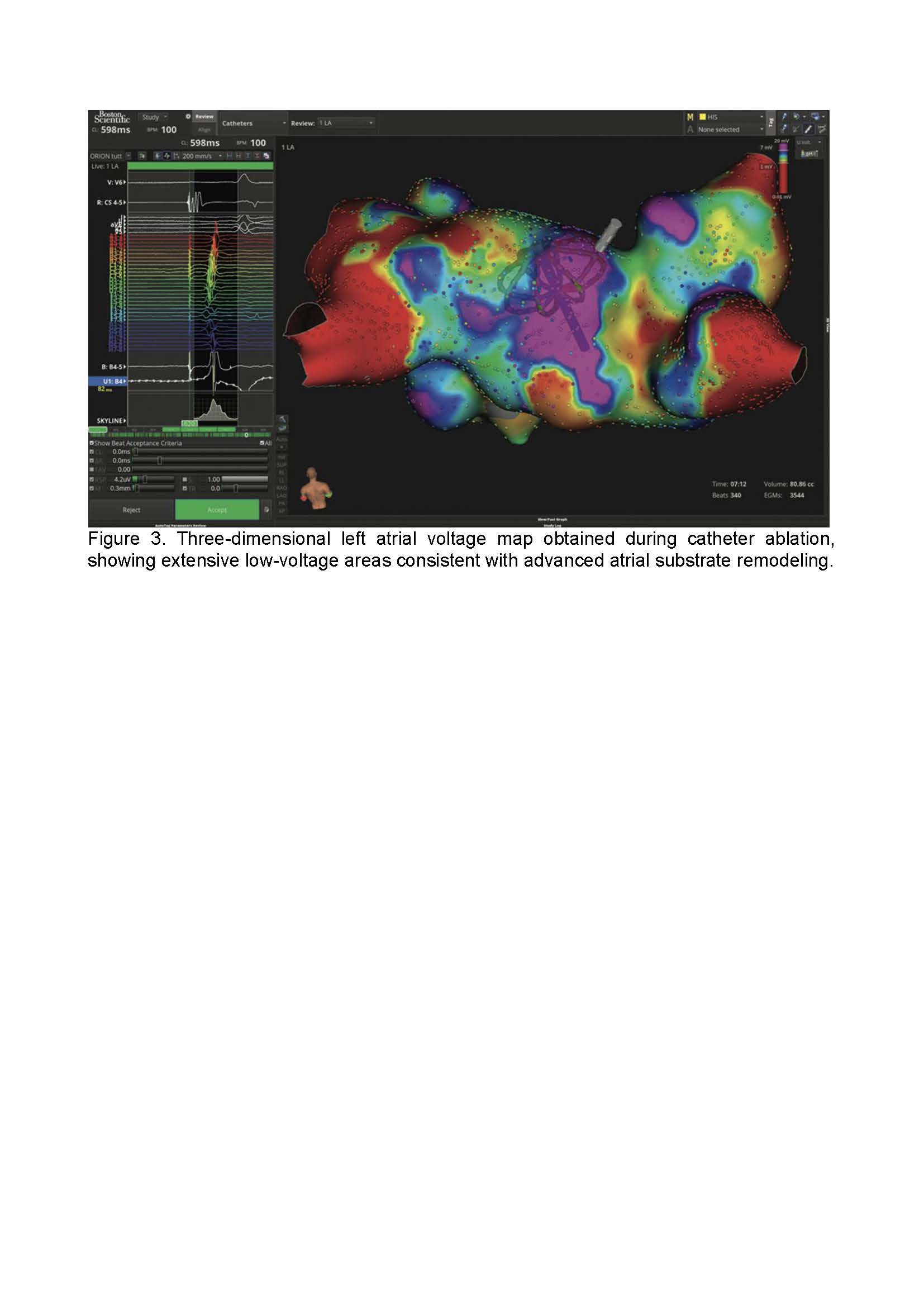
Background: Management of paroxysmal atrial fibrillation (PAF) requires careful selection of rhythm control strategies based on symptom burden and underlying atrial substrate. Clinical risk scores provide useful guidance but do not fully capture atrial structural, mechanical, and electrical remodeling. Advanced echocardiography may offer incremental value for individualized therapeutic decision-making. Methods: We report a case series of three patients with symptomatic or incidentally detected PAF who underwent comprehensive transthoracic echocardiographic evaluation, including left atrial volume assessment, speckle-tracking–derived atrial strain analysis, and tissue Doppler imaging–derived atrial conduction time (PA-TDI). Echocardiographic findings were integrated with clinical features to guide treatment strategy selection. Results: In a patient with structurally normal atria, preserved atrial strain, and normal conduction time, early catheter ablation resulted in sustained sinus rhythm during follow-up. In a second patient with obesity, increased epicardial adipose tissue, reduced atrial strain, and prolonged PA-TDI, a substrate-oriented ablation strategy was required after failure of initial pulmonary vein isolation. In an elderly patient with moderate atrial remodeling, minimal symptoms, and relevant comorbidities, a conservative approach with rate control and anticoagulation was favored, with stable clinical outcome. Across cases, atrial strain and PA-TDI correlated with disease complexity and influenced therapeutic decisions. Conclusions: Advanced echocardiographic assessment of atrial mechanics and conduction provides valuable insights into atrial substrate heterogeneity in paroxysmal atrial fibrillation. Integration of atrial strain and PA-TDI into routine evaluation may support personalized management strategies, optimizing patient selection for catheter ablation and avoiding unnecessary invasive procedures.