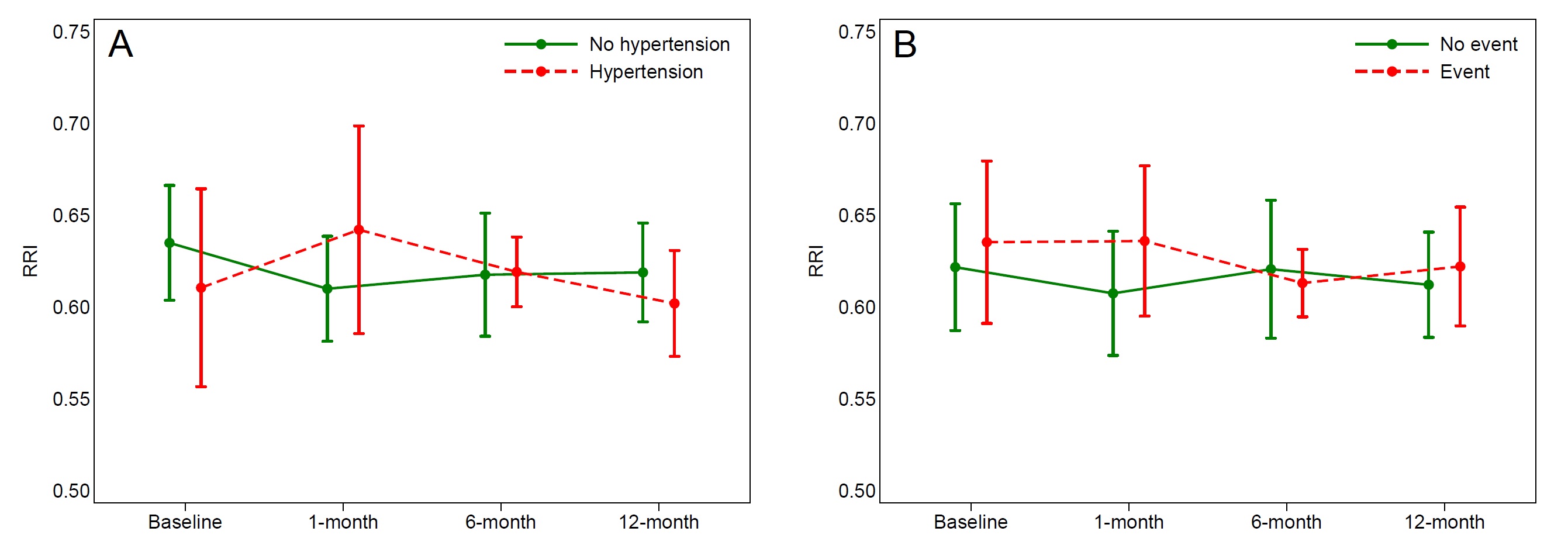
Background : Fluoropyrimidines are the most commonly used drugs in the treatment of colorectal tumors. The fluoropyrimidine-related cardiotoxicity remains a major clinical problem. Purpose: The aim of this study was to evaluate the relationship between cardiotoxicity (CT) and Renal arterial Resistance Index (RRI) as marker of renal perfusion. Methods : One hundred and two outpatients with a first diagnosis of localized or metastatic colorectal cancer were consecutively enrolled. The patients underwent a cardiological evaluation before the beginning of chemotherapy regimen containing fluoropyrimidines. All patients underwent: a clinical evaluation; a routine bloodchemistry to evaluate glomerular filtration rate (GFR) by creatinine (MDRD formula); a blood sample (approximately 3 mL) collected in EDTA-stabilized tubes, according to standard clinical practice, for genetic analysis of variants in fluoropyrimid in metabolism genes known to be associated with cardiotoxicity risk; a transthoracic echocardiogram to assess left ventricular ejection fraction (LVEF) and estimate central venous pressure; a renal echo-Doppler in order to evaluate RRI. Peak systolic and end-diastolic velocity of segmental renal artery were obtained by pulsed Doppler flow and RRI was subsequentely calculated. Results: The overall mean age was 68±10 years. Of the 108 patients included in the study, 49(48%) were male and 51(52%) were female. In the studied population we observed a mean RRI equal to 0.625±0.081 at baseline assessment. We found a statistically significant inverse correlation between RRI and baseline GFR (Pearson r=−0.272, p=0.030). Thirty one patients completed the one-year follow-up. Among them, 30% experienced a significant increase in blood pressure; Additionally, acute coronary syndromes requiring revascularization and hospitalizations for heart failure were observed in 6% and 8% of patients, respectively. Figure shows RRI mean values with 95% confidence interval at baseline and at each follow-up by occurrence of hypertension and cardiac events (panel A and B). Although RRI seems higher in patients with events during follow-up, no significant association was detected. Conclusions: Integrating RRI assessment with fluoropyrimidin e metabolic profiling may enhance the identification of patients at increased risk of cardiotoxicity. Further studies will be needed to clarify the role of the renal resistive index in this setting.