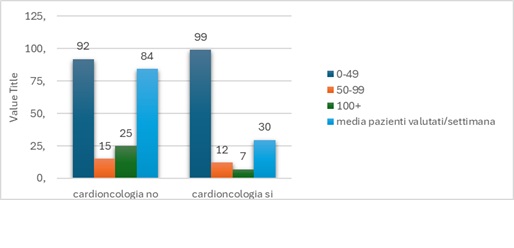
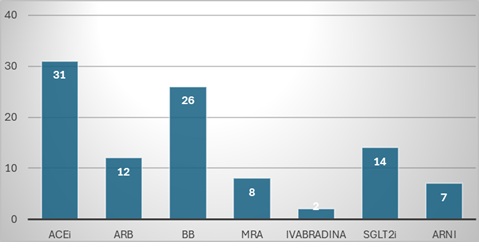
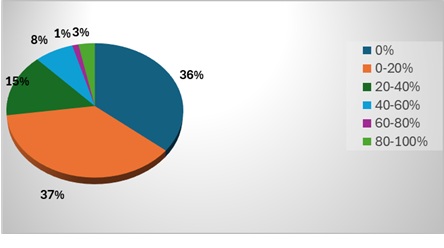
Background: Cardiovascular toxicity could potentially limit anticancer therapy and its features encompassed many different clinical scenarios. Among others, cancer therapy–related cardiac dysfunction (CTRCD) with left ventricular (LV) systolic impairment could represent a major issue. CTRCD is frequently asymptomatic and often effectively treated with standard heart failure (HF) therapy. Limited evidence is available on the need to stop or continue HF therapy after recovery of LV function. The MATCH survey aimed to investigate the real-world approach of Italian cardiologists to this clinical dilemma. Results: The survey was conducted during the 56 th ANMCO National Congress in May 2025. Among more than 2,000 contacts, 250 complete responses from cardiologists were analyzed. 52% of responders reported the lack of a dedicated cardio-oncology service despite managing a higher weekly volume of cancer patients compared with specialised centers (84 vs 29 patients/week) (Fig 1). Two-dimensional echocardiography (2D Echo) was the preferred diagnostic tool for CTRCD in 85% of cases, mainly based on LV ejection fraction (LVEF) assessment, whereas only 10% relied on biomarkers. Angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), and sodium–glucose cotransporter-2 inhibitors (SGLT2i) were the most frequently prescribed therapies (31%, 26%, and 14%, respectively) (Fig. 2). Only 3% of cardiologists reported discontinuing HF therapy after recovery of LVEF in over 80% of patients (Fig 3), usually >1 year after recovery. Discontinuation was primarily guided by cardiovascular risk stratification according to the 2022 ESC Guidelines, and 80% recommended reassessment of LVEF 3–6 months after therapy withdrawal. Few patients required re-start of therapy due to recurrent systolic dysfunction, mainly those at high cardiovascular risk or undergoing further potentially cardiotoxic anticancer treatments. Conclusions: In Italy, discontinuation of HF therapy after asymptomatic CTRCD is uncommon. Patients needs (as pregnancy planning) should be more and more taken into consideration in this challenging decision making. Prospective randomized studies are needed to define the optimal management of patients with stable recovery of LV function after asymptomatic CTRCD.