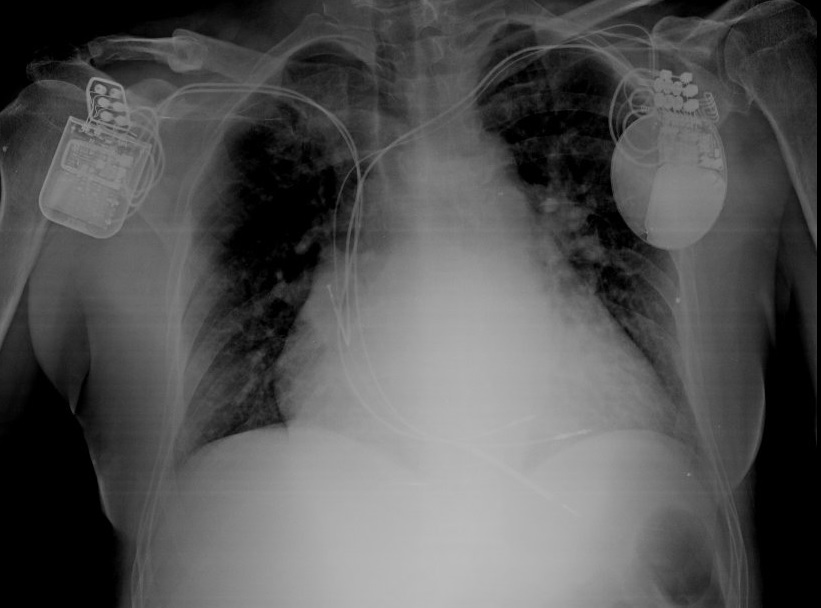
Introduction: heart failure is associated with high mortality rates, that become higher in patients with frequent hospital admissions. Patients with HF and ESKD can be tricky to treat as they’re not eligible for the newest medical therapies, require a multidisciplinary approach and face a higher mortality risk. Case report: A 60-year-old female smoker was admitted to our hospital in January 2024 with an anterolateral STEMI treated with PTCA and DES implantation on the LAD and subsequently on RCA and Cx. Upon discharge EF was normal. Her medical history included ESKD for which she had been on daily peritoneal dialysis for about 10 years but with some residual renal function. In April 2024 she was admitted to our ward with acute pulmonary oedema. A transthoracic echocardiography showed moderate left ventricular dilation with severe systolic dysfunction, aneurysmal dilation of the apex and mildly reduced RV function. At admission she was on DAPT, low dose bisoprolol and MRA. Ticagrelor was discontinued due to acute anemia requiring blood transfusions. The medical therapy couldn’t be further titrated because of hypotension and episodes of complete AV block. We decided to implant an ICD in primary prevention, without performing a MRI and a new coronary angiography. In June, she was hospitalized for worsening dyspnoea. At the end of August she was readmitted for acute pulmonary oedema complicated by ACC secondary to non-shockable rhythm, successfully resuscitated. A TTE showed severe systolic and diastolic dysfunction, moderate to severe MR and RV dysfunction. After clinical stabilization, she underwent coronary angiography that showed no intra-stent restenosis. We started treatment with dapaglifozin, although with an off label dispensation. In September 13, we implanted a CCM device. In November, during the follow-up visit, she was euvolemic (NYHA I-II), without clinical signs of heart failure. The patient had a significant improvement in quality of life. She has been evaluated as an outpatient at our transplant centre and considered too frail for L-VAD and not a candidate for a kidney-heart transplantation as she is now in NYHA class I-II. Conclusions: our clinical case highlights the role and efficacy of dapaglifozin and CCM in improving quality of life, NYHA class and reducing re-hospitalizations in a patient with ESKD and heart failure, like a bridge therapy that has delayed the need to list the patient for transplantation improving her daily life.