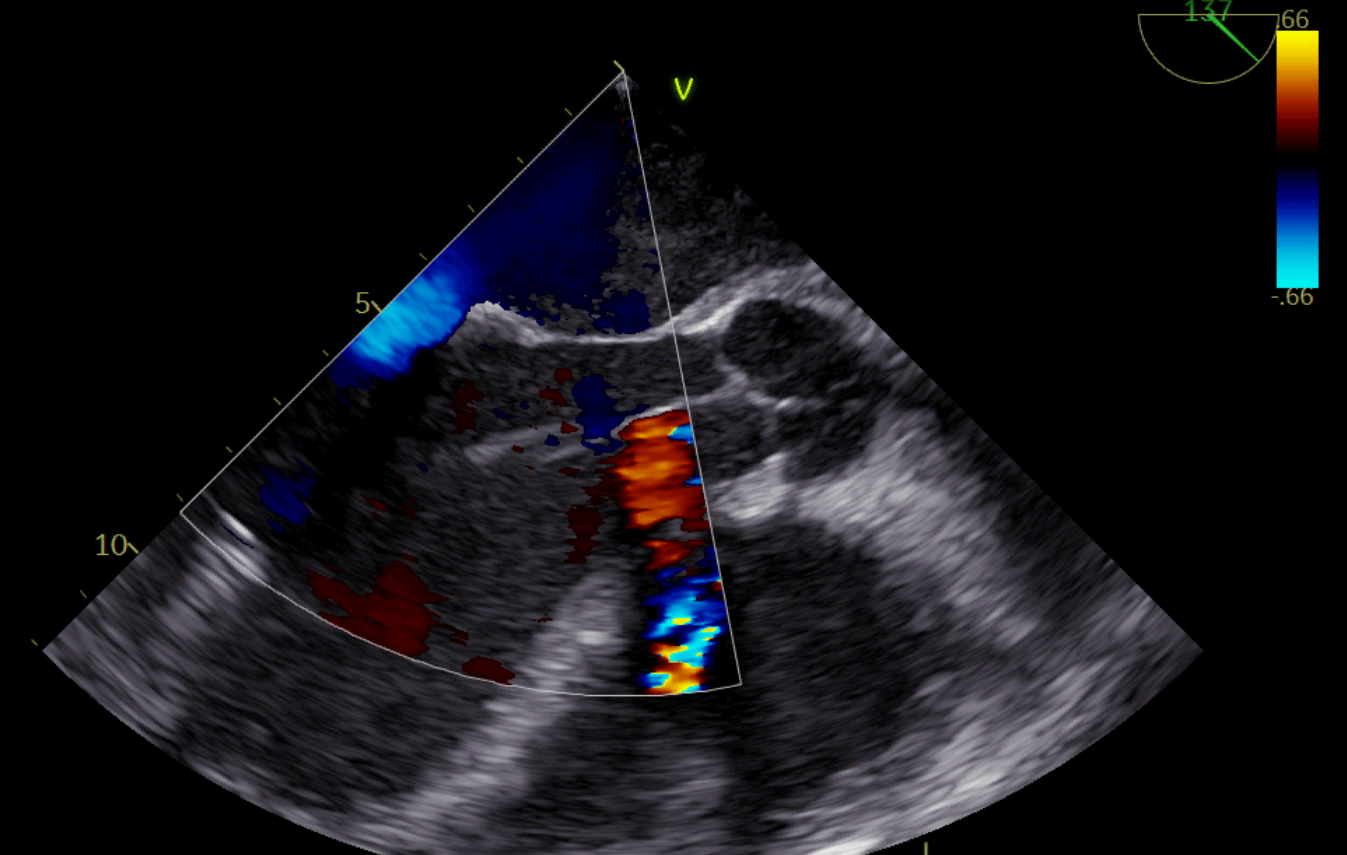
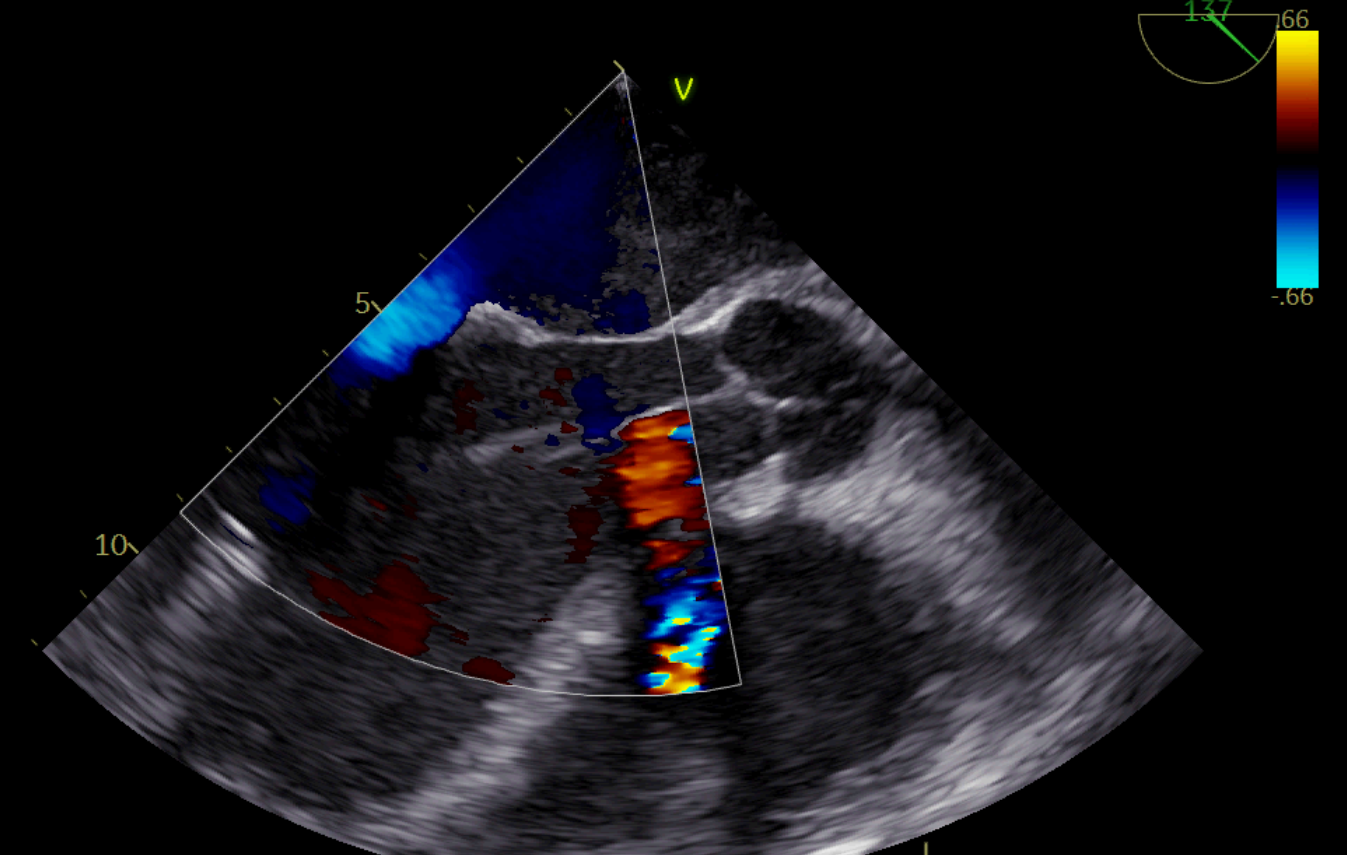
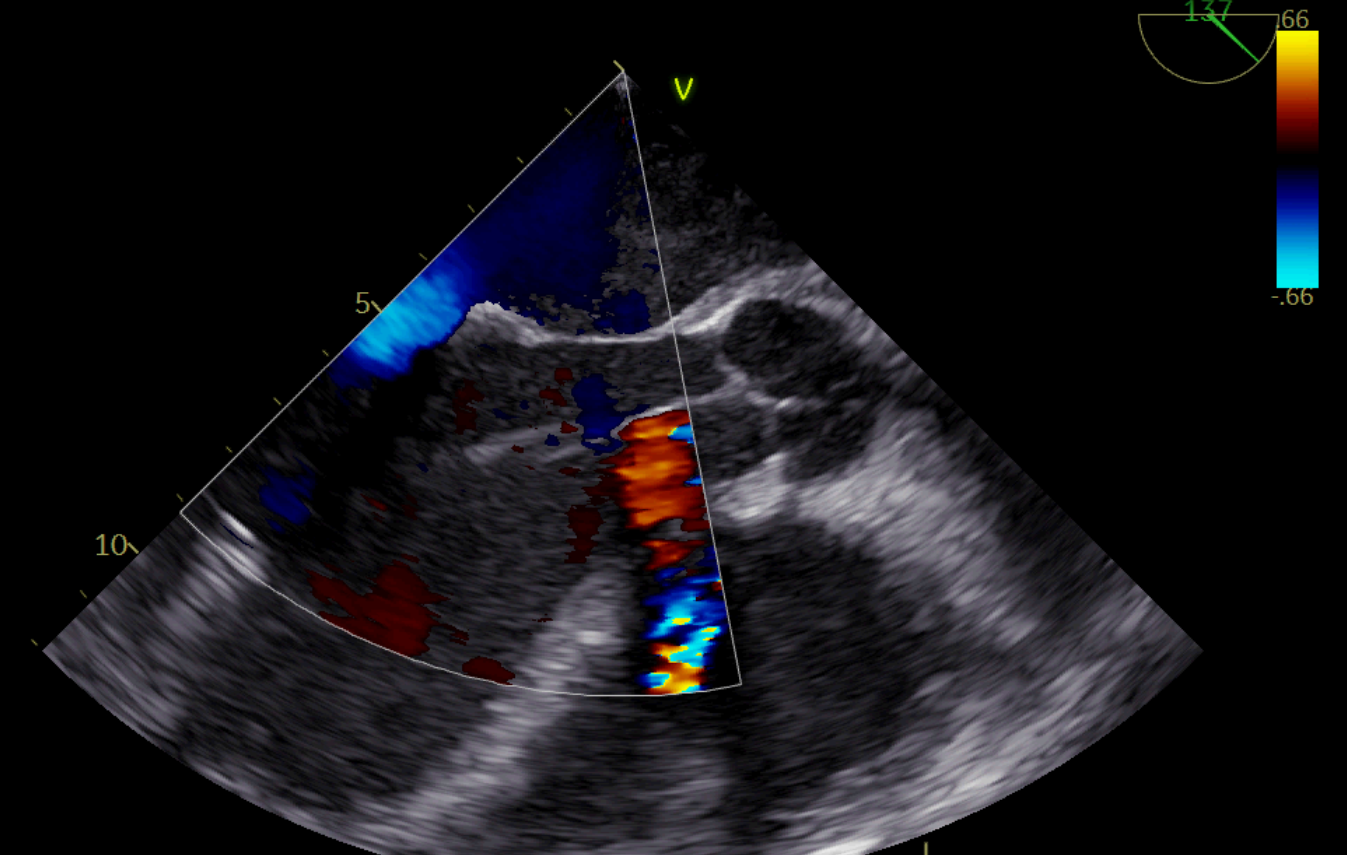
B.D, male, 46 years old, suffering from idiopathic dilated cardiomyopathy (DCM) with advanced biventricular involvement, treated with current guideline-directed medical therapy, bearer of S-ICD, previous percutaneous mitral edge-to-edge repair. He accesses our ER for exacerbation of heart failure secondary to atrial fibrillation (AF). Within a few days, because the patient's AF was not responsive to either rate control or rhythm control, he developed stage C cardiogenic shock according to SCAI classification, so he was admitted to the post cardiac surgery intensive care unit of our AORN. Hemodynamics was supported with inodilators and inoconstrictors and IABP, until he developed acute tubular necrosis that required treatment with continuous venovenous ultradiafiltration (CVVHD) for about two weeks. Having recovered renal function, the patient was placed on the transplant list in the macro-area urgency class. The patient's echocardiographic picture at that point included severe biventricular systo-diastolic dysfunction (LVEF 15%, RV FAC 15%, grade III diastolic dysfunction, moderate degree residual mitral insufficiency), with a severe splanchnic congestion state. Hemodynamic parameters showed post-capillary pulmonary hypertension with preserved cardiac output, on multiple vasoactive medication (PAPm 44mmHg, PCWP 34mmHg, CI 2.85L/min/m2, PVR 1.75 WU). Although the patient presented biventricular dysfunction, in order to attempt to relieve right ventricular afterload by effective unloading of the left ventricle, an Impella 5.5 device was implanted by axillary artery as a bridge to transplant. Impella was maintained for 21 days, and both the transesophageal echocardiogram during implantation and subsequent transthoracic echocardiograms did not observe any improvement in right ventricular function, nor in splanchnic congestion status, which was also confirmed by hematochemical tests. Therefore, following discussion in the Heart Team and with the patient and his family members, it was decided to implant a total artificial heart (TAH, Aeson, Carmat). The patient was extubated the morning after surgery, and after 5 days of therapeutic adjustment in the ICU, he was transferred to the ward after a total ICU stay of two months. Conclusion: Total artificial heart implantation is a therapeutic option in patients with advanced biventricular heart failure refractory to other medical and/or interventional therapies with the aim of bridge to transplant.