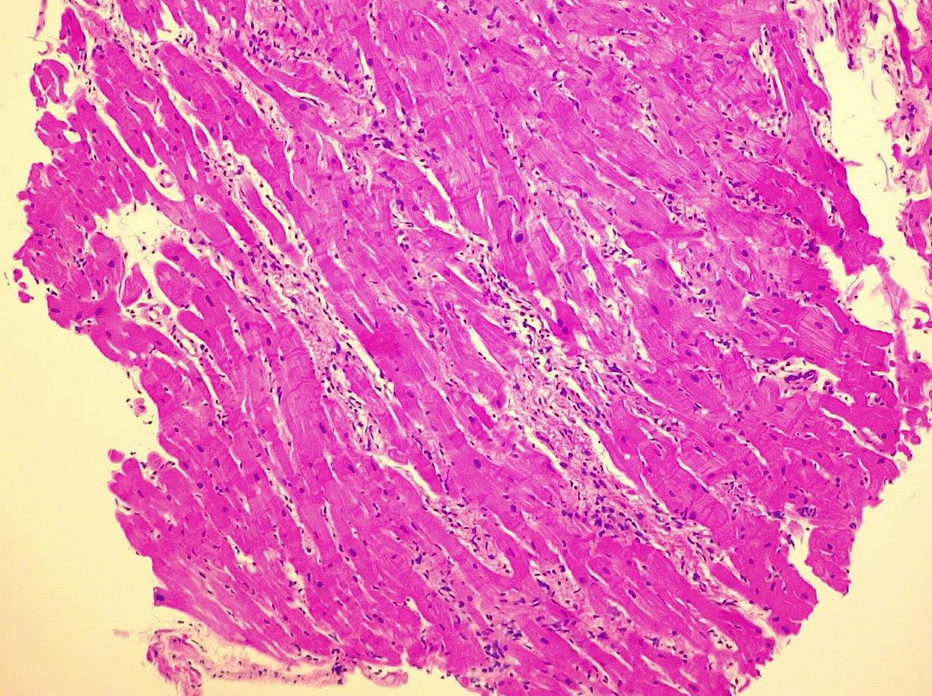
Female, 31 years old, in May 2024, while on her honeymoon in Santo Domingo, was stung by an unspecified insect. Upon her return, after about a week, she develops fever unresponsive to home therapy therefore she accesses the infectious emergency room of our AORN, where she is found to have IgG antibodies against chikungunya (CHIK) virus, in the absence of the viral genome. After a few days, she developed tetrahyposthenia for which brain CT scan found cerebral hemorrhage of the great falx cerebri without any indication for neurosurgery. For markes elevation of myocardionecrosis, we practiced an echocardiogram. We found severe reduction of left ventricular function (LVEF 35%) with global hypokinesia, particularly in the inferolateral wall, diastolic dysfunction grade III and severe mitral insufficiency. Therefore, she was transferred to our UTIC, where hemodynamics was supported with inodilators and vasodilators, respiratory failure managed with CPAP. We performed an endomyocardial biopsy the day after with findings of active myocarditis, in the absence of viral genome detection. On abdominal ultrasonography there was suprahepatic veins thrombosis. Therefore, autoimmune screening was being sought. A diagnosis of systemic lupus erythematosus and antiphospholipid antibody syndrome was being made. The patient thus started therapy with Hydroxychloroquine, Methylprednisolone and low molecular weight heparin. Progressively there was improvement in the neurological picture, once hemodynamic stability was achieved, optimized medical therapy (OMT) for heart failure was introduced. Pre-discharge right heart catheterization presented with postcapillary pulmonary hypertension with preserved cardiac output (PAPm 33mmHg, PCWP 20mmHg, PVR 1.9WU). Cardiac MRI showed diffuse active myocardial damage (high T1 values), diffused subendocardial and transmural LGE at the inferolateral wall. The patient was discharged with progressive improvement in echocardiographic data (LVEF 44%, grade II diastolic dysfunction, mild-to-moderate mitral insufficiency) on HF OMT, rheumatology therapy, and antithrombotic therapy with VKA. Currently, the patient is being followed by a multidisciplinary team and has presented no heart failure-related events. Conclusion: Because the genome of CHIK virus was never found, we hypothesized that antibody positivity to the virus was a secondary event to the antiphospholipid antibody syndrome and that the insect bite was a confounding anamnestic finding.