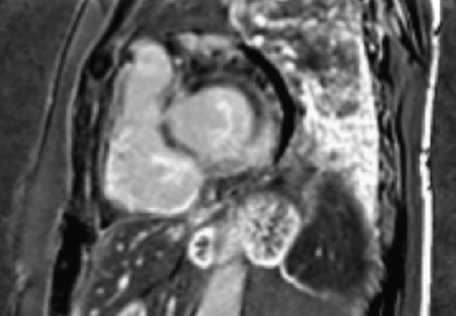
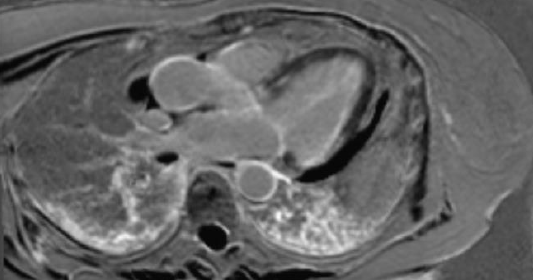
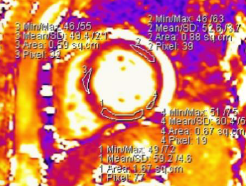
Case report: A 56-year-old woman with history of hypertension and MGUS (IGM kappa) presented with syncopal episodes, hypotension, exertional dyspnea and asthenia. The patient was admitted to our Cardiology ward due to elevated NTProBNP and hs troponin (1500 ng/l, vn <14); the coronary angiography showed normal coronary arteries. Transthoracic echocardiogarphy (ETT) revealed mild hypertrophy of the interventricular septum (IVS) with preserved biventricular kinesis. AL Amyloidosis (aAL) was suspected and confirmed by abdominal fat biopsy: it showed focal interstitial deposits of fibrillar substance referable to amyloid, positive on immunoelectromicroscopy for kappa light chains. The patient was then admitted to the Hematology ward to start chemotherapy, but spondylodactylitis, skin thickening and narrowing of the oral fissure were detected. Systemic Sclerosis (ScS) was then suspected and confirmed with laboratory tests (positivity of ENA anti-Scl70), so mycophenolate was started. The patient was then evaluated by the cardiac amyloidosis team: the ETT showed a slight thickening of the IVS (11 mm) and circumferential pericardial effusion but associated with a-dyskinetic areas in the inferior-posterior segments of left ventricle (LV). Considering the wall motion abnormalities not typical for cardiac amyloidosis, an endomyocardial biopsy was performed. This examination confirmed the presence of focal amyloid deposits but associated with strips of connective tissue and doubtful myocyte necrosis and lympho-monocytic infiltration on histological examination. First-line therapy for aAL was started (Daratumumab, Bortezomib, Cyclophosphamide and Dexamethasone), with sudden reduction in hs troponin (300 ng/l). Cardiac MRI was then performed to evaluate the prevalent structural cardiac alteration between aAL and ScS. The exam showed extensive fibrosis of both ventricles, with transmural extension in basal infero-posterior wall of LV, compatible with diffuse ScS myocarditic involvement. Bortezomib was then suspended due to its potential cardiotoxicity during myocarditis and the dosage of immunosuppressive therapy was adjusted. A progressive reduction in TnHs (23 ng/l) and NT-proBNP values and improvement of symptoms was then observed. Discussion and conclusions: The integrated use of cardiovascular imaging and biopsy examinations guided by an expert cardiomyopathies team is essential for a correct classification of patients with overlapping conditions.