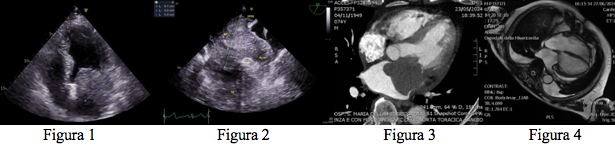
CLINICAL CASE: A 73-year-old man, a former smoker, came to the emergency department for speech disturbance and deviation of the oral rhyme compatible with ischaemic cerebral stroke (brain CT scan excluded haemorrhagic phenomena). The ECG showed new atrial fibrillation while the transthoracic echocardiography showed a voluminous inhomogeneous ovoid mass in the left atrium (fig.1 ) inducing severe mitral stenosis (mean G 10 mmHg); the subsequent transesophageal echocardiographic examination confirmed the presence of a voluminous mass completely occluding the left auricle and a large part of the left atrium with extension towards the mouth of the left superior pulmonary vein in the absence of a clear plane of cleavage with the cardiac walls (fig. 2). A fully diagnostic CT heart scan with mdc was performed which confirmed the presence of the left atrial mass of about 8 cm in diameter occupying the auricle and a large part of the atrium with inhomogeneous densitometry and progressive moderate enhancement with foci of neoangiogenesis (fig.3 ), MRI of the heart showing pathological tissue that was inhomogeneously iso-hyperintense in T1 and hyperintense in T2 with heterogeneous and progressive enhancement, maximum in late phase, and a coronarography scan showing critical coronary artery disease of VATS. The patient underwent removal of the atrial mass, reconstruction of the roof of the left atrium and the origin of the left superior pulmonary vein with bovine pericardium, mitral anuloplasty with Memo3D 28 ring, single aorto-coronary bypass (left AMI on VATS), amputation and suture of the left auricle. Histopathological analysis was positive for a malignant connective tissue neoplasm, extensively necrotic and haemorrhagic, with a spindle morphology, hypocellular myxoid areas and compact hypercellular areas, compatible with intimal sarcoma with a high degree of replication and deserving of adjuvant chemotherapy. Subsequent echocardiography and post-operative heart MRI showed no residual lesions or significant valve regurgitation (Fig. 4). CONCLUSIONS: the clinical case highlights once again the incidental diagnosis of intracavitary cardiac masses, even large ones, which in the above-mentioned case was possible following ictal neurological symptoms secondary to cardiac embolism. It is therefore essential to include cardiac imaging in clinical brain manifestations of ictal character for a precise and correct aetiological definition of the disorder.