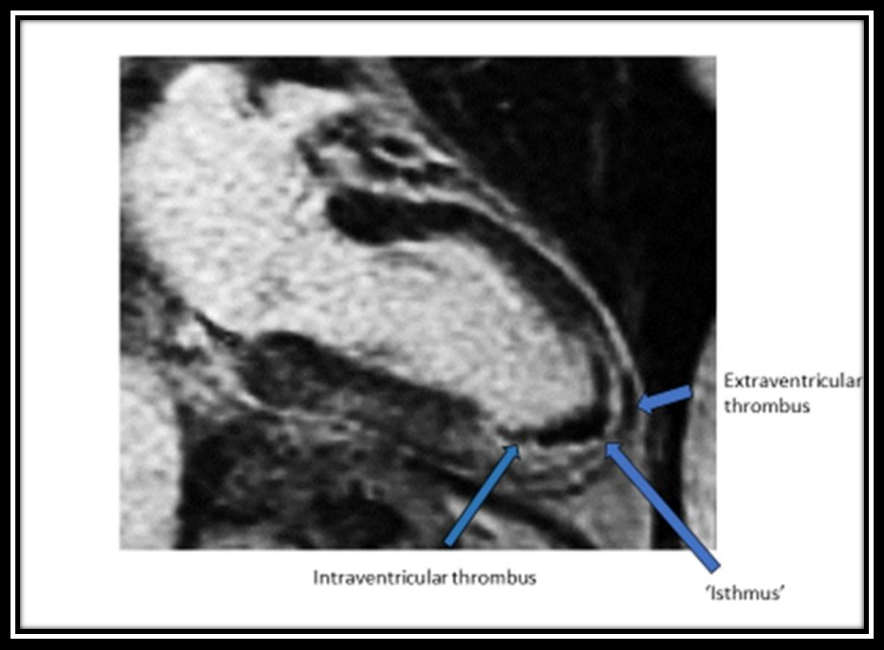
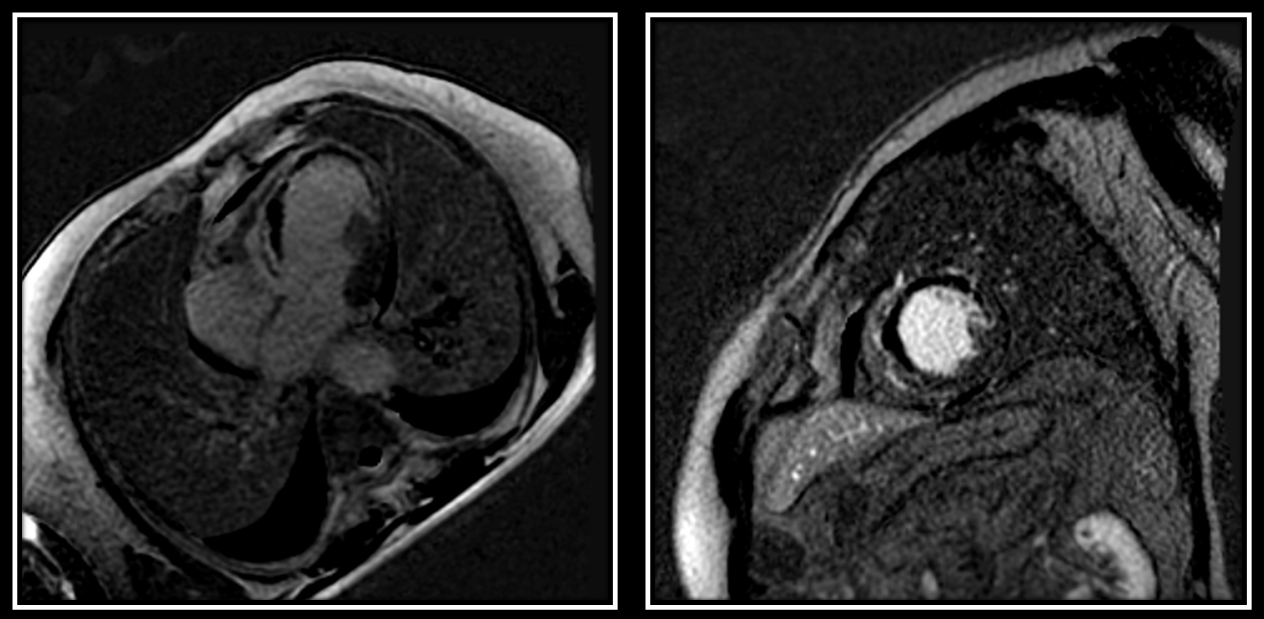
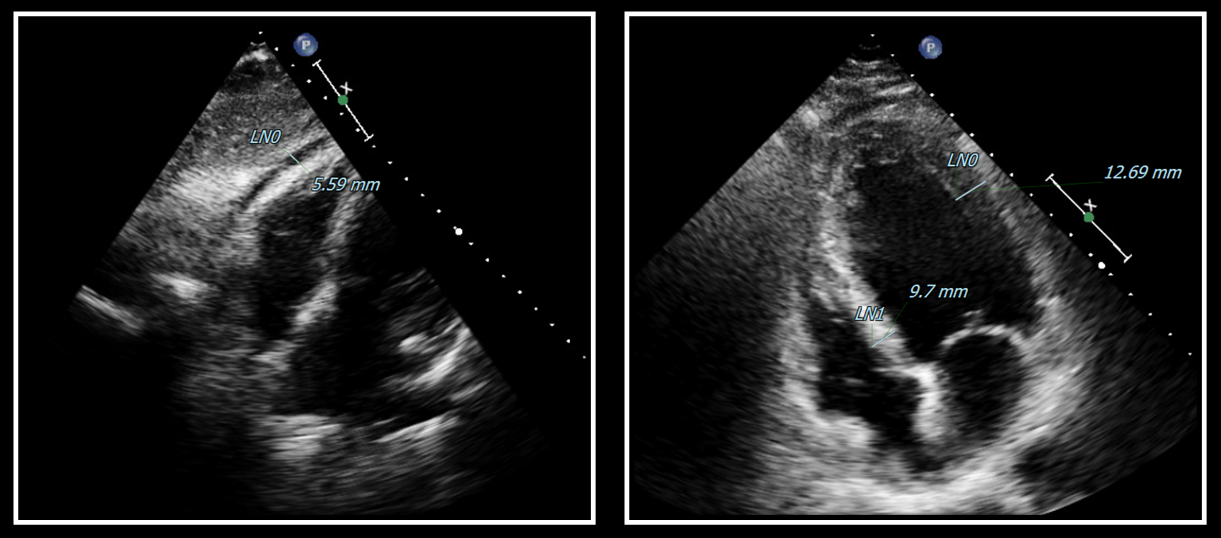
Background Heart rupture (HR) is a rare but highly lethal complication of STEMI, yet the ability of CMR to predict progression to overt rupture in high-risk patients remains unexplored. Purpose To derive CMR-based predictors of Impending or Covered Heart Rupture (ICHR) and to prospectively validate whether a composite risk model can be reconstructed using transthoracic echocardiography in high risk STEMI patients. Methods We conducted a two-phase study including a multicenter retrospective derivation cohort undergoing early post-reperfusion CMR (n=205) and a single-center prospective echocardiographic validation (n=68). Comprehensive CMR tissue characterization was performed. ICHR was adjudicated as transmural MVO, Extramyocardial thrombus and Ventricular pseudoaneurysm. In the prospective cohort, the derived Rupture Risk Triad (RRT) was reconstructed echocardiographically (eRRT), and tested against CMR. Results In the retrospective cohort, 26 patients (12%) fulfilled CMR criteria for ICHR. ICHR was associated with universal MVO and IMH, increased infarcted wall thickness, elevated infarcted-to-remote wall thickness ratio, and frequent pericardial effusion (PE). On univariate analysis, max infarcted wall thickness (OR per 1mm increase 1.57, 95% CI 1.30–1.90; p<0.0001), infarcted-to-remote wall thickness ratio (OR 1.40, 95% CI 1.25–1.63; p<0.0001), LV thrombus (OR 6.3, 95% CI 2.5–15.0; p=0.001), and PE (OR 45.0, 95% CI 13–161; p<0.0001) were strongly associated with ICHR. Combined into the CMR-derived RRT, defined by PE, max infarcted wall thickness >12 mm, and infarcted-to-remote wall thickness ratio >1.1, a strong association with ICHR (OR 371, 95% CI 68–2036; p<0.0001) emerged, being the only independent predictor on multivariable analysis (OR 263, 95% CI 28–2512; p<0.0001; AUC 0.90). In the prospective cohort of high risk STEMI patients with PE, the eRRT demonstrated an overall accuracy of 86.8%, and was strongly associated with CMR-confirmed ICHR (OR 34.4, 95% CI 8.2–144.4; p<0.0001). Of 21 patients with CMR-confirmed ICHR, 2 underwent urgent ventriculoplasty and 5 required emergent pericardiocentesis for tamponade; all effusions were hemorrhagic. Conclusions The CMR-derived Rupture Risk Triad (cRRT) identifies STEMI patients at high risk of progression to overt cardiac rupture and can be reliably reconstructed using routine echocardiography (eRRT), providing a pragmatic bedside tool for early risk stratification and timely escalation of care.