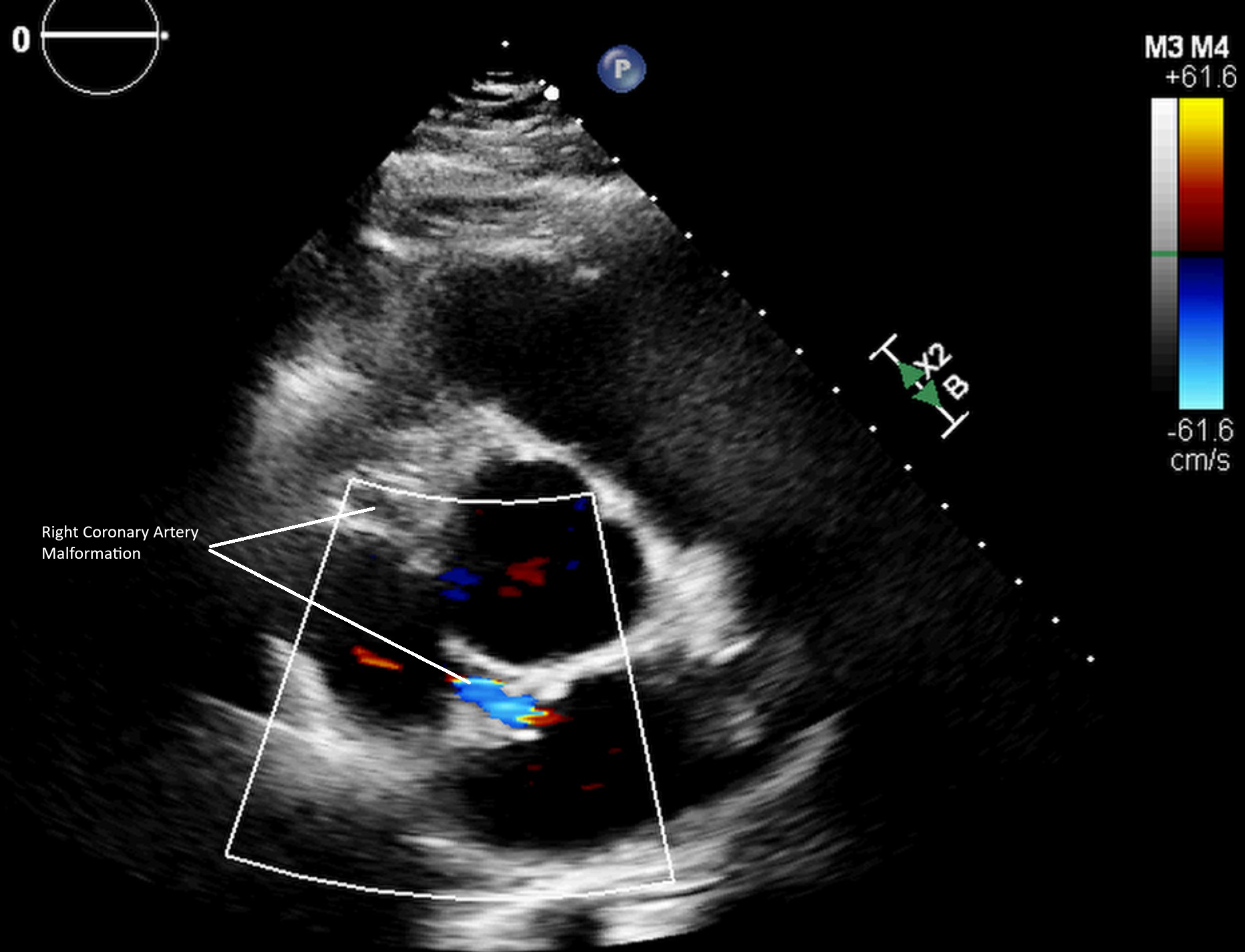
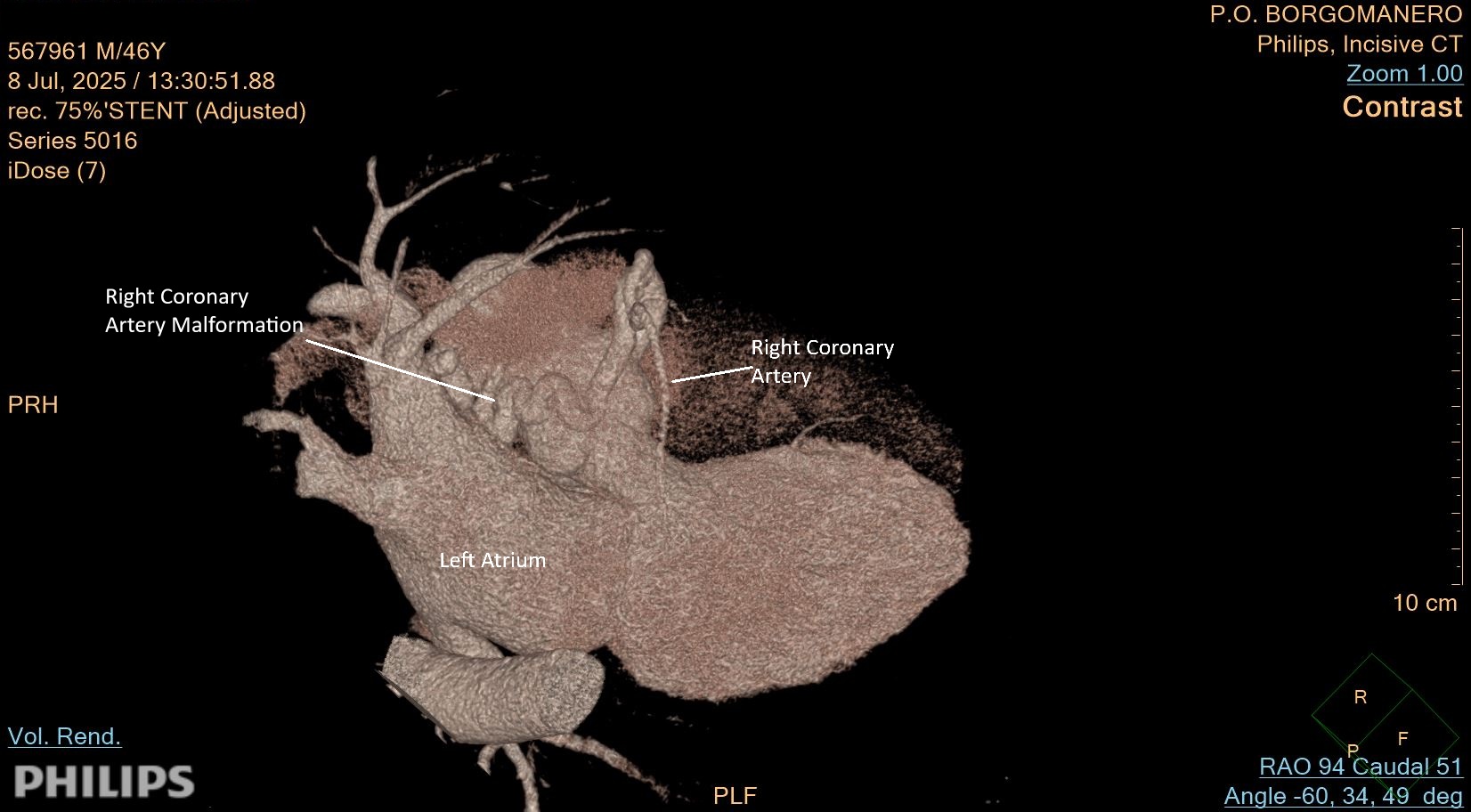
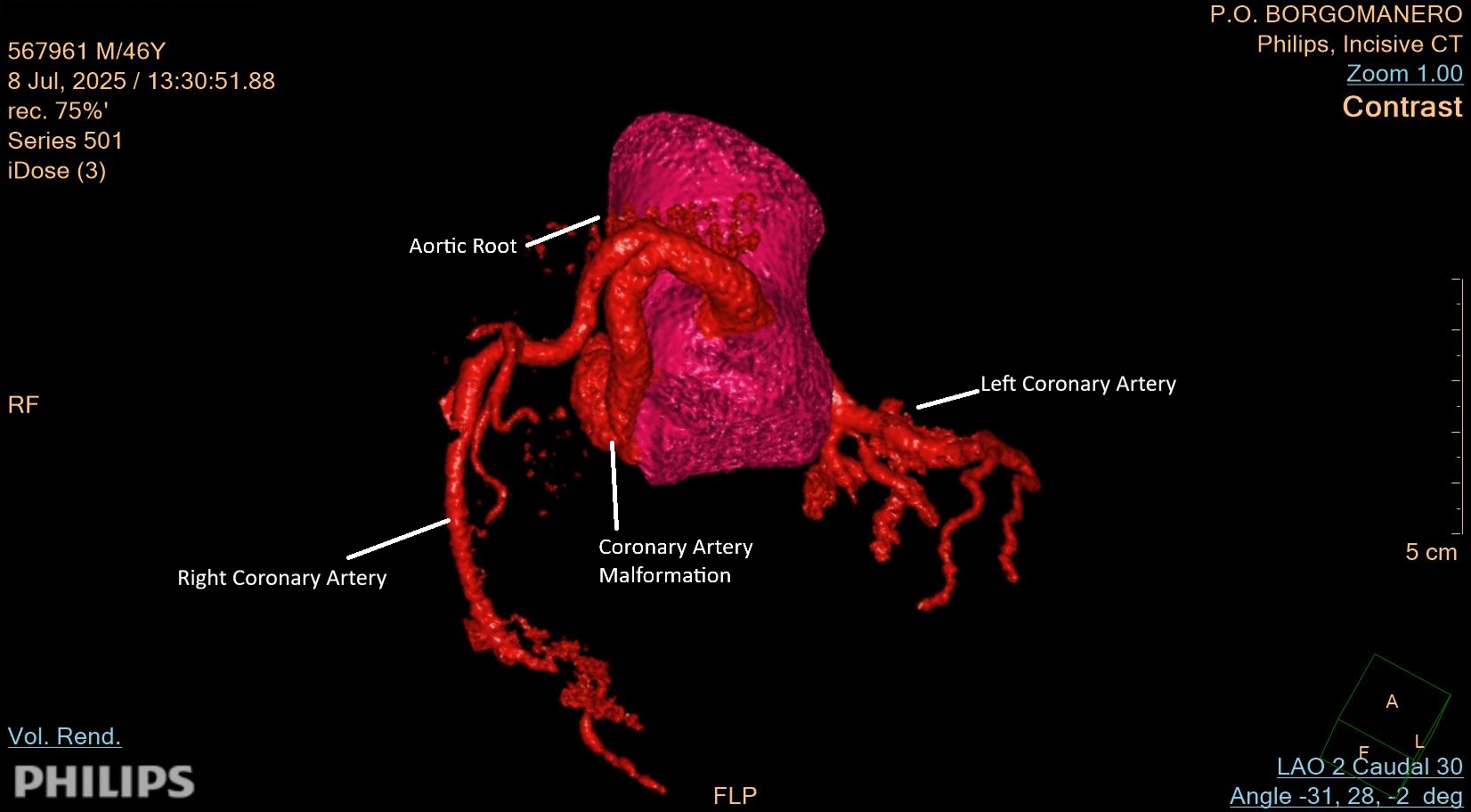
We present a case of a men fortysix years old, with hypertension and Von Hipple-Lindau syndrome (VHL), rare inherited autosomal dominant genetic disorder, that predisposes to the formation of benign and malignant tumors in various parts of the body, such as angiomas in the retina and cerebellum (hemangioblastomas), renal tumors (renal cell carcinoma), pancreatic and adrenal cysts (pheochromocytomas) and vascular malformation. It is caused by a mutation in the VHL gene, which impairs the control of cell growth, and requires regular monitoring and a multidisciplinary approach for the management. He has undergone bilateral nephrectomy in 2013 for renal neoformation, since then on dialysis. In 2017 a cerebellar hemangioblastoma was removed. He has also pancreatic neoformation NET G1 in followup. Executed cardiologic evaluation for possible renal transplant; in January 2025 he performed negative maximal ergometric test. Asymptomatic during normal daily activities. Ecocardiogram showed dilated, slightly hypertrophic left ventricle, with preserved systolic and diastolic function, dilated left atrium and normal-sized right chambers, mild ectasia of the aortic root and ascending tract; in parasternal short axis view abnormal flow is detected, apparently direct to the left atrium, referrable to a probable abnormal right coronary artery course (fig. 1); mild mitro-tricuspid regurgitation, normal pulmonary pressure, absence of pericardial effusion. At the coronary CT scan there was no significant coronary stenosis; from the proximal segment of the right coronary artery emerges a very dilated and tortuous branch that probably flows into the right atrium suspected for arterious malformation. (Fig 2,3) Executed coronary angiography that confirmed epicardial coronary arteries without significant stenosis, voluminous fistula originating from the proximal tract of right coronary artery projecting into the left atrium; distal artery with normal caliber and vascularization. The case was discussed with clinical indication for imaging follow-up and medical therapy. This interesting case shows how a systemic disease must be studied with a multidisciplinary approach for the possible involvement of multiple organs. This is a rare case of coronary malformation in the context of VHL syndrome, where vascular malformations in other organs are described but not in the heart; ecocardiography and CT scan are essential for diagnostic and therapeutic decision and follow-up.