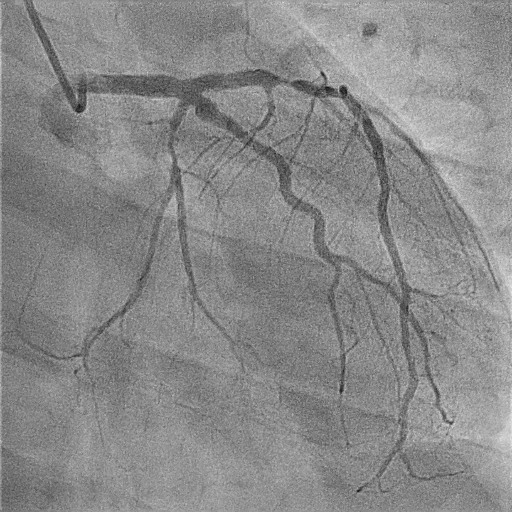
Prevalence of Heterozygous Familial Hypercholesterolemia (FH) is estimated to be around 1/200-250, which corresponds to 14-34 million cases worldwide. A 27 years-old man was referred to our clinic because of exercise angina. He had a total cholesterol (TC) of 379 mg/dl, HDL 38 mg/dl, LDL 330 mg/dl and TG 150 mg/dl. During the bicycle stress test, he reported chest pain, which was associated to inconclusive ST changes on the ECG. A stress echocardiography showed regional wall abnormalities of the left ventricular apex, associated to symptoms. Contractile abnormalities and symptoms disappeared in the recovery period, thus indicating the presence of myocardial ischemia. He was therefore put on aspirin, highly intensive statin and betablocker. He was then admitted to our cardiology ward to perform a coronary angiography, which showed a three vessels disease with sub-occlusion of the middle left anterior descending artery (LAD), a critical stenosis of the proximal Left Circumflex (Cx) artery and a moderate stenosis of the proximal Right Coronary artery. The PCI of LAD and Cx with drug eluting stent implantation was then performed. At discharge, the lipid panel still showed high cholesterol levels (TC: 249 mg/dl, LDL: 214 mg/dl), despite high dose of atorvastatin. Three of the patient’s first-degree relatives (mother, father, and sister) suffered from premature coronary artery disease. No tendon xanthomas/xanthelasmas were found at physical examination, but a severe bilateral “arcus cornealis”. Dutch-Lipid Score was 15, suggesting a definitive diagnosis of heterozygous FH. The patient was put on triple lipid lowering therapy, combining evolocumab, atorvastatin 80 mg and ezetimibe. After 3 months the Patient’s cholesterol values decreased dramatically (TC: 99 mg/dl, LDL: 30 mg/dl). He remained completely asymptomatic for the following 5 years, with LDL levels always lower than 40 mg/dl. Recently the patient was admitted again to the cardiology ward because of unstable Angina and coronary angiogram showed a “de novo” severe stenosis of distal LAD, not suitable for PCI or stenting. LDL was only 29 mg/dl. After treatment with PCSK 9 inhibitors, high doses statin and ezetimibe the Patient had an optimal regression of LDL values, reaching the target of < 40 mg/dl. Despite the good laboratory results, he experienced a second cardiovascular event. The still unresolved question in patients with FH is: when our best clinical practice is not effective, what else can we do?