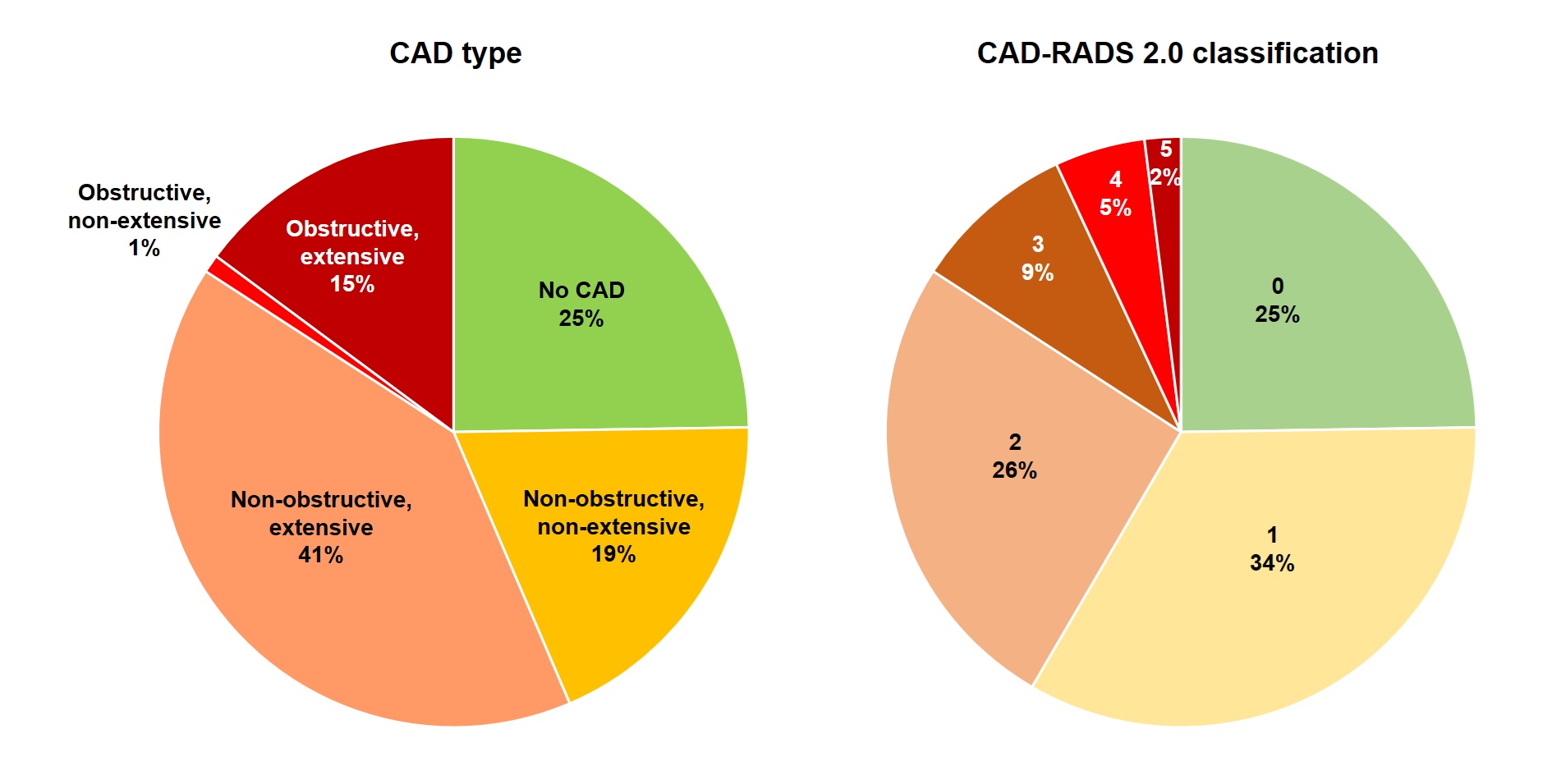
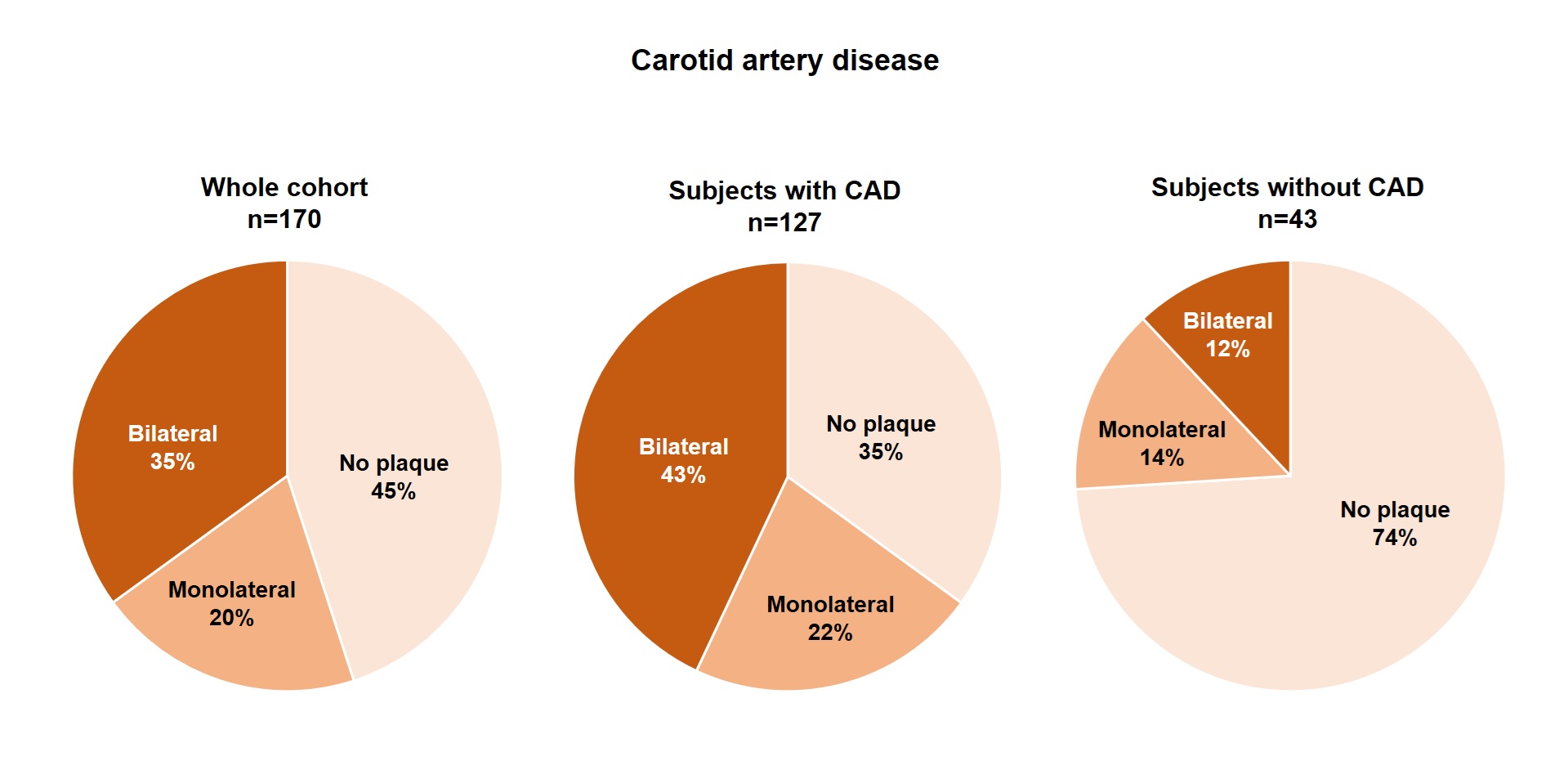
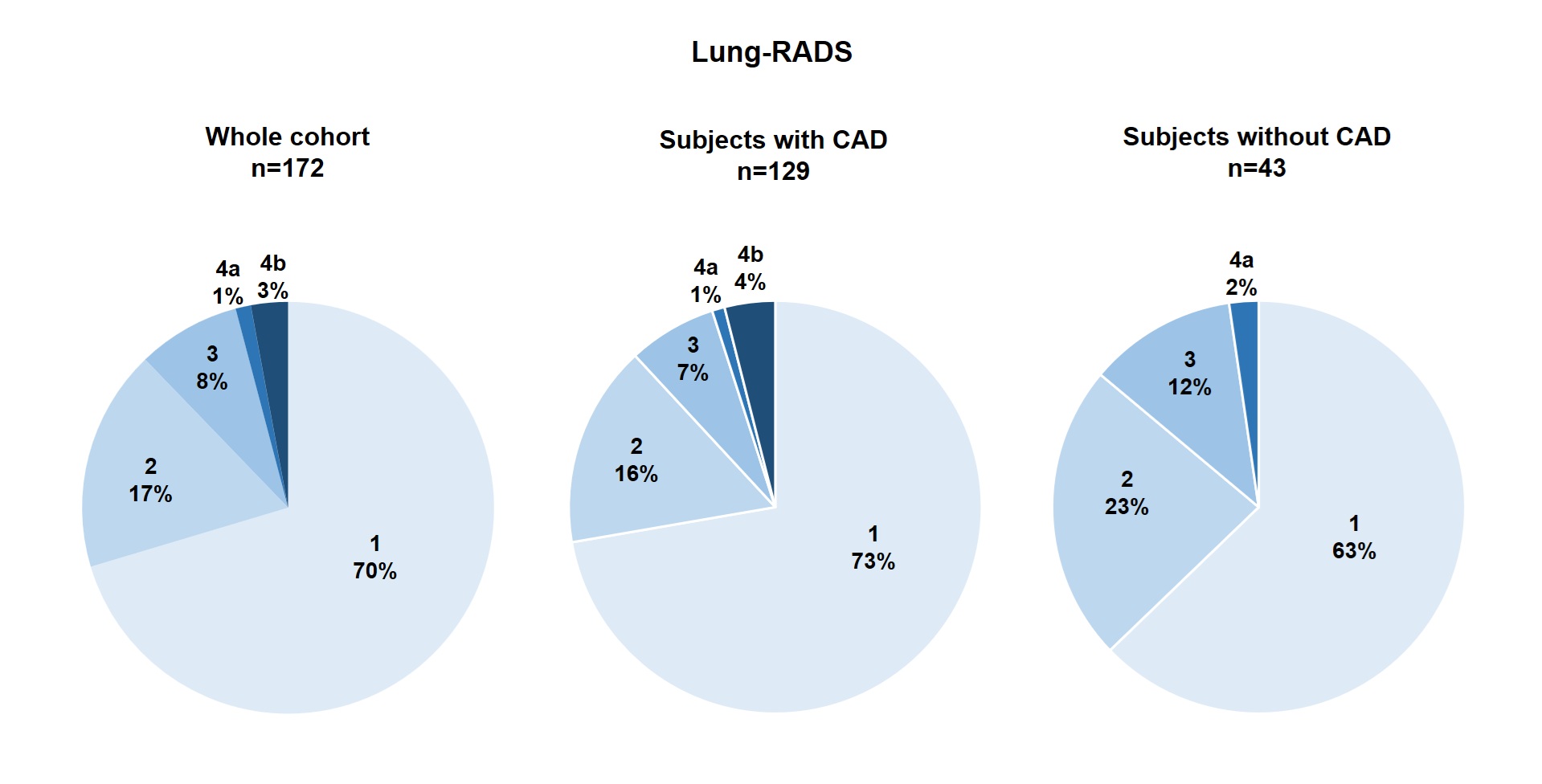
Background: Photon-counting computed tomography (PCCT) enables high-resolution, multiorgan vascular and thoracic imaging. We tested whether a single-visit PCCT screen can uncover subclinical, clinically actionable disease in asymptomatic, high-risk adults. Methods: Prospective, general practitioners (GP)-directed cohort of adult subjects aged 45–75 years meeting ≥1 criterion: type-2 diabetes for ≥10 years, current or former smoking (who had quitted <15 years), or Framingham Risk Score for Hard Coronary Heart Disease ≥10%. Key exclusions were typical angina or angina-equivalent symptoms, prior coronary/carotid CT/angiography, cardiomyopathy, iodinated-contrast allergy, and chronic kidney disease. Participants underwent a PCCT protocol covering coronary arteries, thorax, and carotids (effective dose 11–13 mSv). This interim analysis spans enrolment from 11 January to 21 June 2025; outcomes included prevalence/severity of coronary atherosclerosis, carotid plaque burden, Lung-RADS category, incidental findings, downstream referrals, and therapy changes. Results: PCCT was completed in 172 participants (median age 62 years [interquartile range 54–68]; 56% male) without adverse events. Any coronary atherosclerosis was found in 129 (75%), and obstructive CAD (corresponding to at least one stenosis ≥50%) in 25 (15%). Coronary artery disease was classified as non-obstructive, non-extensive in 32 (19%), non-obstructive, extensive in 71 (41%), obstructive, non-extensive in 1 (1%), and obstructive, extensive in 25 (15%). Eight participants (5%) were referred for invasive coronary angiography; to date, 4 (2%) underwent percutaneous coronary intervention and 2 (1%) coronary artery bypass grafting. Carotid plaques were identified in 94/170 evaluable scans (55%), and were bilateral in 60/170 (35%). Thoracic findings included Lung-RADS 3–4 nodules in 21/172 (12%) and emphysema in 41/172 (24%). Incidental extra-thoracic work-ups included one papillary thyroid carcinoma confirmed after ultrasound-guided evaluation. Following PCCT, antiplatelet therapy was initiated in 62%, lipid-lowering therapy in 45% and up-titrated in a further 22%. No adverse events attributable to PCCT were recorded. Conclusions: In high-risk asymptomatic individuals, a PCCT screen revealed a substantial burden of clinically actionable atherosclerotic and pulmonary disease, was feasible and safe, and frequently catalysed treatment initiation or intensification with selective invasive assessment.