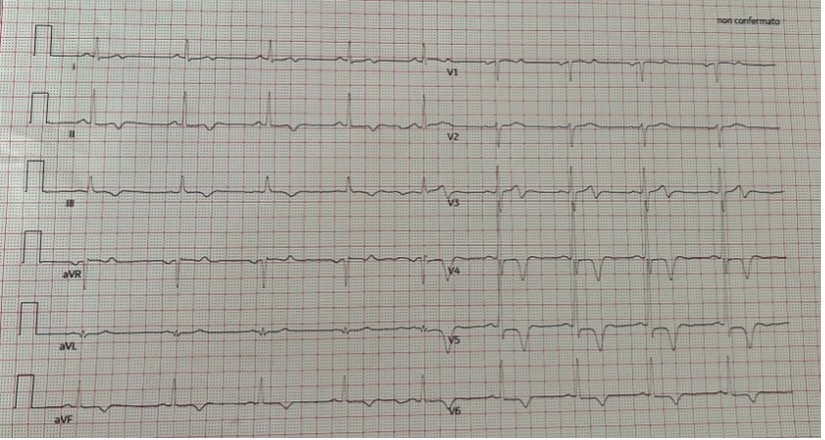
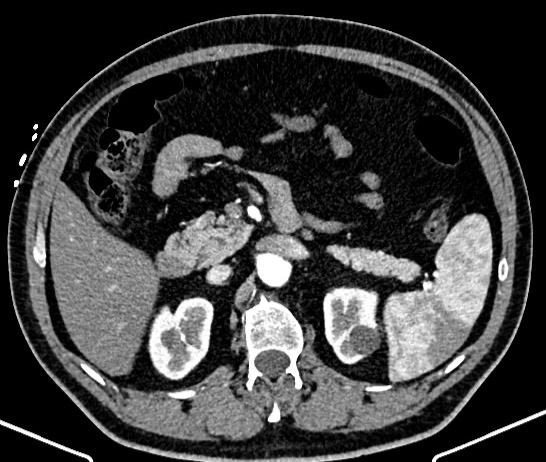
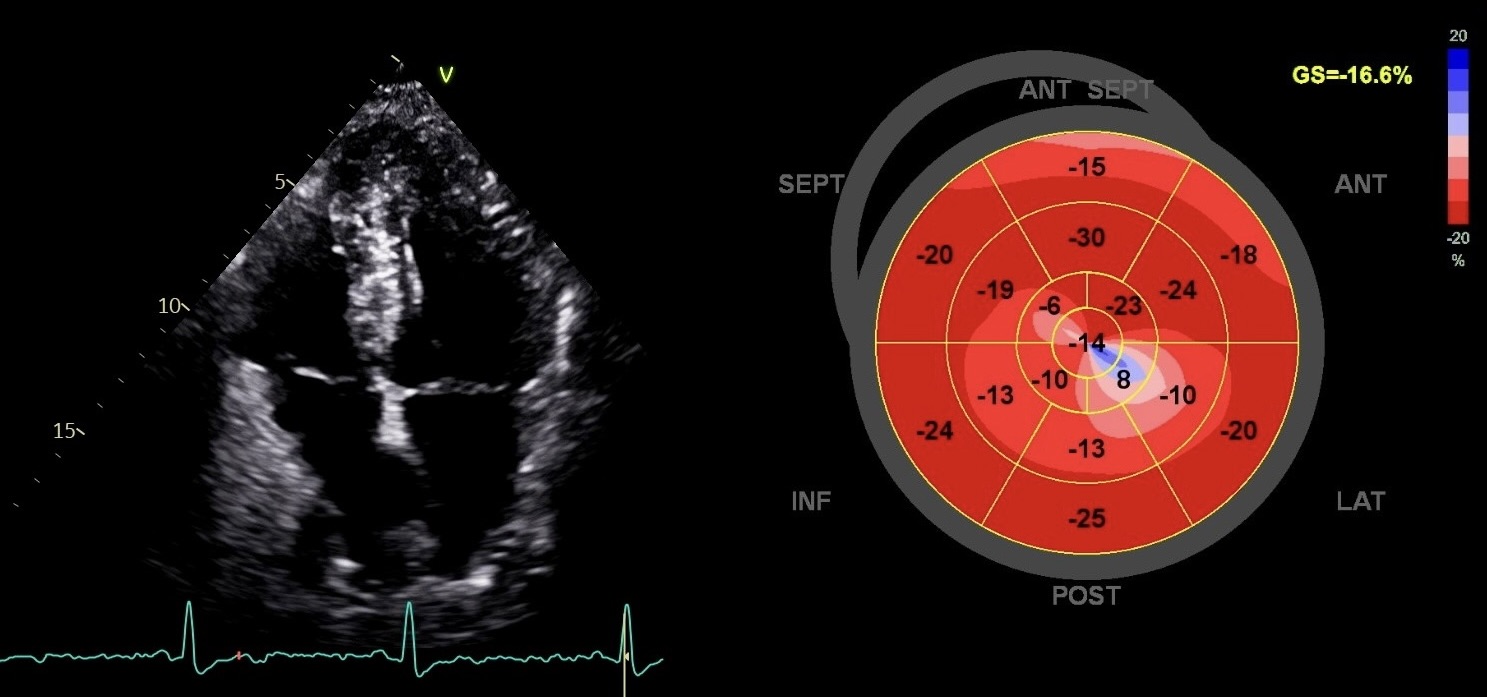
Introduction Acute left-sided abdominal pain radiated to the left shoulder due to splenic infarction can be confused with cardiogenic thoracic pain. Splenic infarction is frequently linked to infiltrative hematologic disorders, but it can be also related to cardioembolic events. We present the case of a patient admitted to cardiology ward because of chest pain and subsequent radiologic evidence of splenic infarction, along with a first diagnosis of hypertrophic cardiomyopathy (HCM) and patent foramen ovale (PFO). Case presentation A 58-year-old man came to our attention complaining chest pain with radiation to the left shoulder associated with profuse sweating. Troponin levels were normal. ECG revealed deep and negative T waves in the antero-lateral leads. CT angiography excluded aortic dissection but revealed a large spleen infarction. Coronary angiography excluded obstructive coronary disease. A transthoracic echocardiogram showed left atrium dilation, asymmetric left ventricle hypertrophy with apical hypokinesia and GLS pattern abnormalities suggestive of HCM. Bubble test confirmed the presence of PFO with moderate to severe right-to-left shunt. Left atrial appendage thrombosis was excluded. Cardiac MRI confirmed HCM without LGE areas. Coagulation disorders were excluded. No surgical intervention for splenic infarction was needed. The patient was treated with acetylsalicylic acid and he was provided with an internal loop recorder to exclude arrythmias before evaluation for PFO closure. Discussion The challenge of this case is represented by splenic infarction etiology. After ruling out hematologic causes and coagulation disorders, thromboembolic causes were investigated. Atrial fibrillation (AF) has been described as a cause of splenic infarction. In this patient, no arrhythmic events were detected during telemetric monitoring. However, HCM can be related to atrial arrythmias, especially if left atrium is dilated. Cardiac MRI excluded left ventricular apical aneurism as possible cause of intracardiac thrombosis, but PFO can represent another confounding factor. There have been episodic reports of splenic thromboembolism in patients with PFO. However PFO, seen in ~25% of the general population, may therefore coexist by chance in a patient with an unexplained left circulation embolism. Therefore, in high-risk patients for AF, a telemetric cardiac monitoring period of six months can be reasonably considered to rule out AF before deciding on PFO closure.