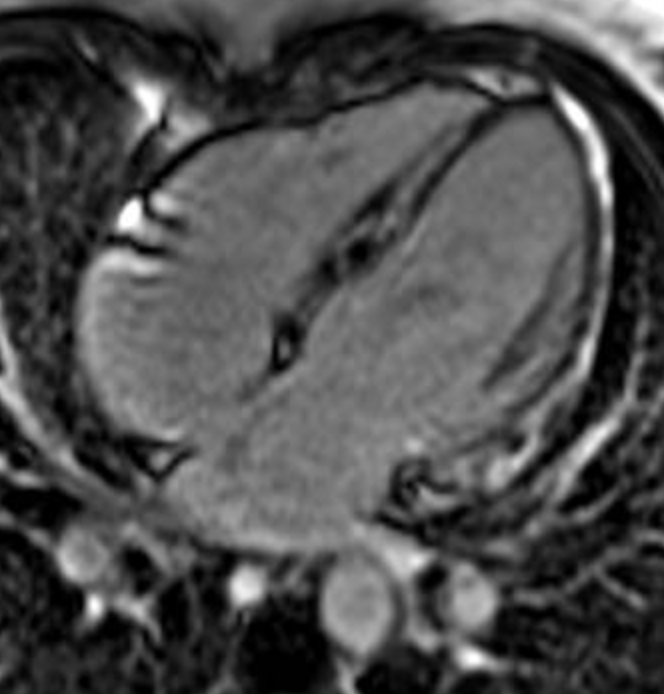
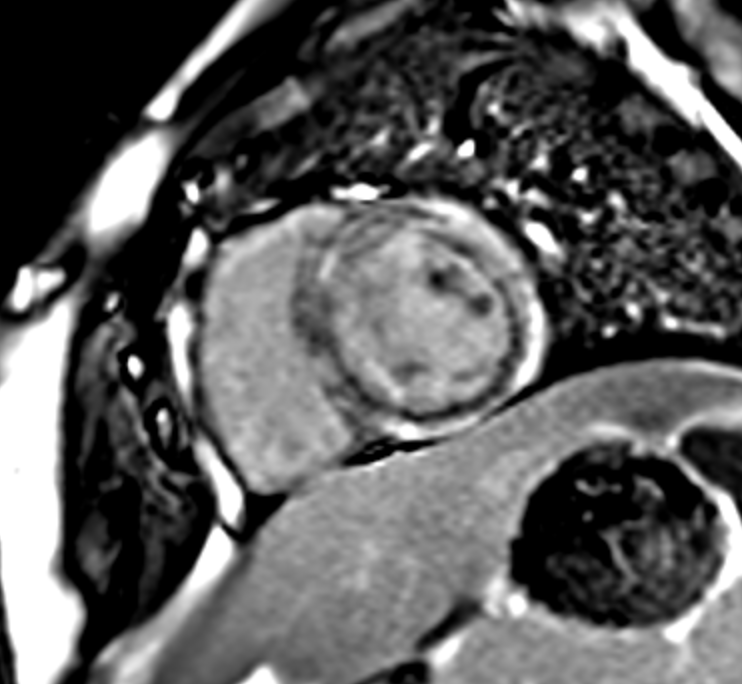
Background and aim: Epidermolysis bullosa simplex (EBS) is a rare inherited blistering disease and mutations in kelch-like protein 24 (KLHL24) were recently implicated in a unique subtype of EBS [1,2]. KLHL24 is expressed at similar levels in keratinocytes and cardiomyocytes. There is a growing association of dilated cardiomyopathy in EBS-KLHL24 that may be severe and usually present in early adulthood. We aim to describe the early pediatric onset of scarring cardiomyopathies (CMP) in EBS-KLHL24 patients. Case reports: We report two cases of pediatric onset of KLHL24 mutation related-CMP: a boy of 13 years old and a girl of 12 years old. Both patients were asymptomatic, and showed at cardiac examinations the presence of mild left ventricular dilatation with preserved ejection fraction on echocardiogram, the ECG holter monitoring and the exercise stress test documented polymorphic ventricular ectopic beats (VEBs). Non-sustained ventricular tachycardia (NS-VT) was also documented in the boy. The cardiac magnetic resonance (CMR) showed in both patients the presence of diffuse biventricular late gadolinium enhancement (LGE). Patients started medical treatment and the boy, due to the presence of NS-VT, underwent also ICD implantation in primary prevention at age of 15 years old. Conclusions: Given the potential of early onset and the rapid progression of the cardiomyopathy, initially presenting with myocardial scars with the associated risk of life threatening arrythmias, routine cardiac screening, including ECG, ECG holter monitoring, exercise stress test and CMR, is recommended since the young age to identify pre-symptomatic patients and timely act preventive measures to improve their outcome.