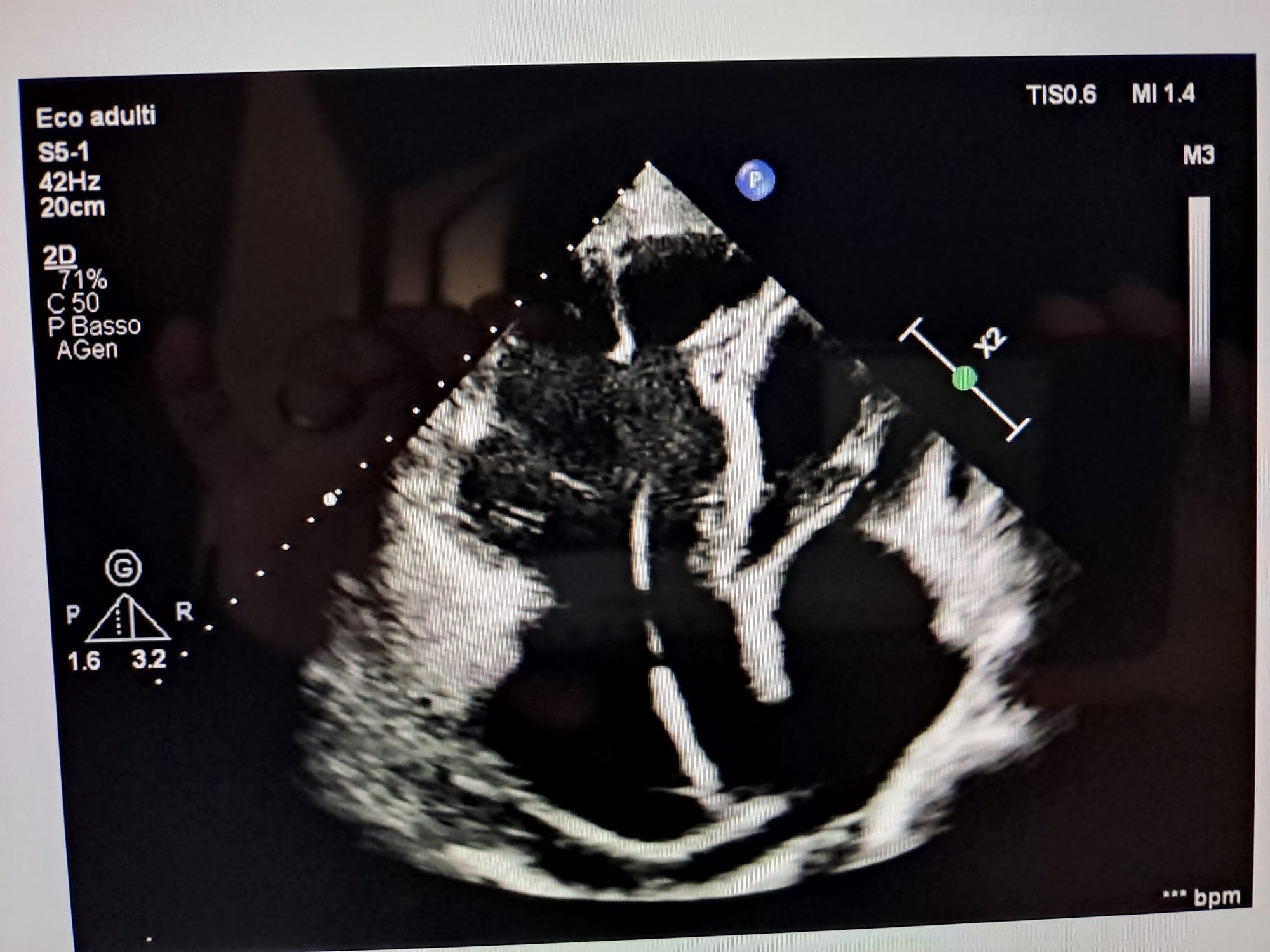
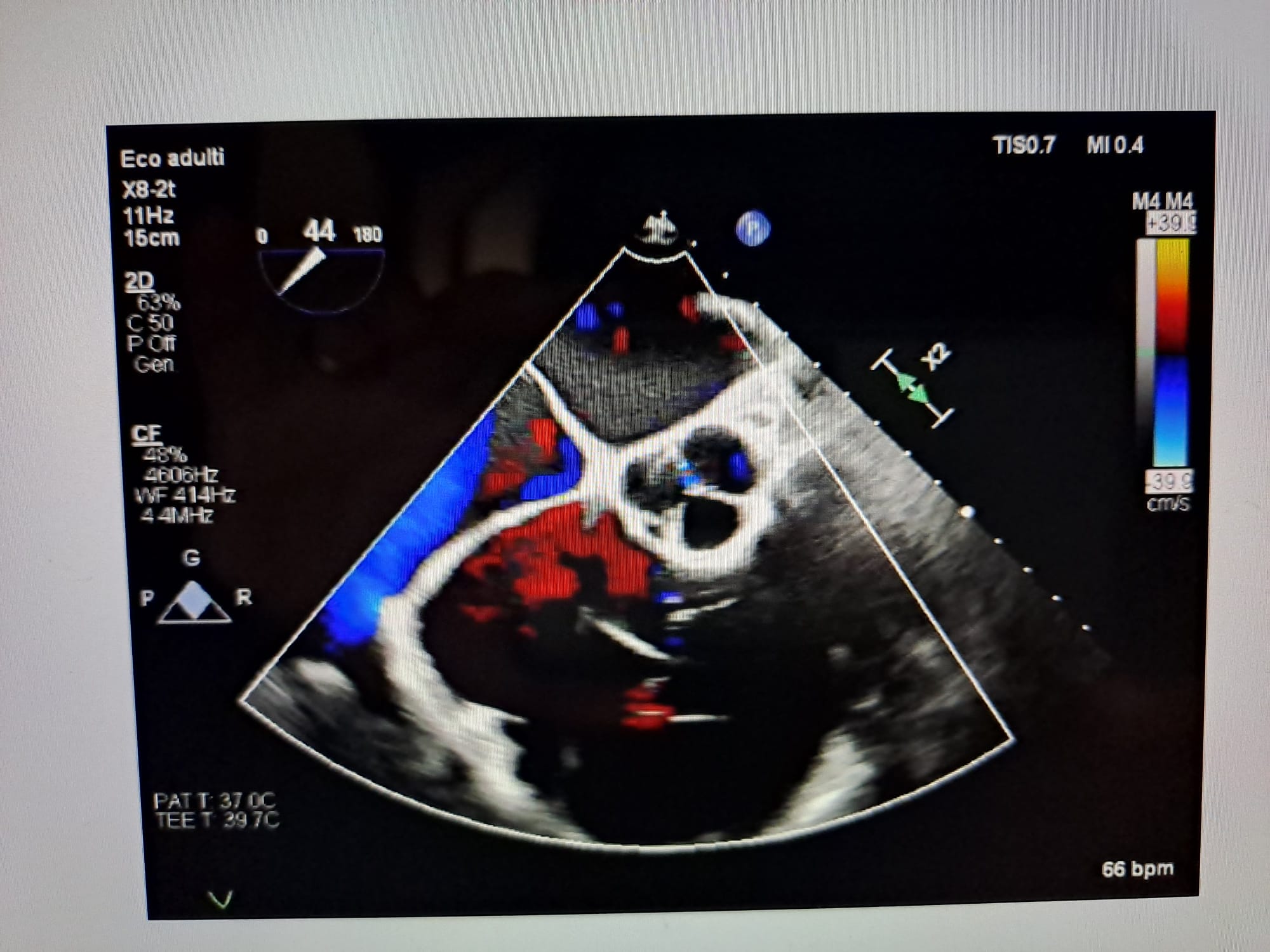
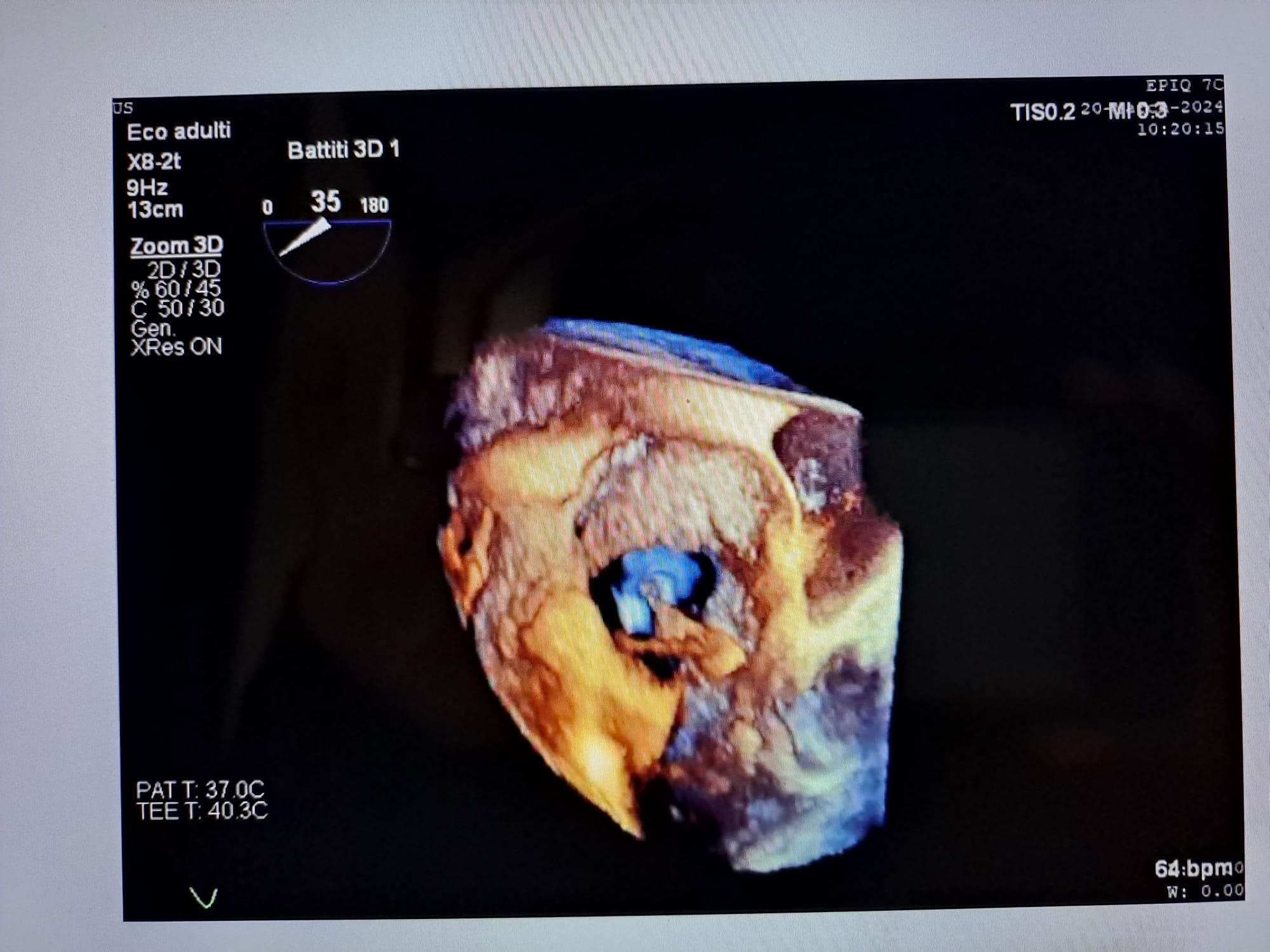
A 71-year-old man labeled in the past as having “arrhythmogenic right ventricular dysplasia” was hospitalized in May 2022 for exacerbation of right-sided heart failure symptoms. He suffered from arterial hypertension and dyslipidemia, he was an ex-smoker and had family history of ischemic heart disease. In 2014 a slow-slow atrioventricular (A-V) node reentrant tachycardia was registered and afterwards a radiofrequency ablation was performed. In 2018 a bicameral pacemaker was implanted to treat episodes of 2:1 and third-degree A-V block with pathological pauses. The transthoracic echocardiogram performed at the time of the hospitalization showed a hypertrophic and not dilated left ventricle, with an ejection fraction (EF) of 40% and a mainly diastolic D-shape; severely dilated right ventricle with highly impaired contractility; giant right atrium; massive tricuspid regurgitation due to complete leaflets coaptation gap; mild pericardial effusion. Decongestion with combination therapy of diuretics and vasodilators led to 17 kg weight loss. Coronary angiography was negative. Upgrading to a right ventricular bifocal stimulation defibrillator was carried out. The patient was discharged in good conditions. During follow-up, in order to evaluate tricuspid valve and interatrial septum in chronic right ventricle overload, a transesophageal echocardiography was performed. The interatrial septum was intact, no shunts were found at this level. The tricuspid valve had a marked dilated annulus (61 mm) and hypoplastic leaflets, causing an almost single right chamber without gradient between ventricle and atrium due to massive regurgitation. The unexpected discovery was a wide membrane in the right atrium compatible with a possible embryonic remnant of the right valve of the sinus venosus. Three-dimensional reconstructions illustrated the membrane going from the anterior wall of the inferior vena cava toward the superior vena cava with insertion at the crista terminalis, dividing the right atrium halfway. A consistent diagnosis of cor triatriatum dexter (CTD) was made, resulting from failure of involution of the right venous valve through the sinus venosus. Furthermore, CTD is sometimes associated with other right heart abnormalities, including tricuspid dysplasia, and with supraventricular arrhythmias. CTD is a rare congenital abnormality that must be ruled out in chronic right ventricle overload.