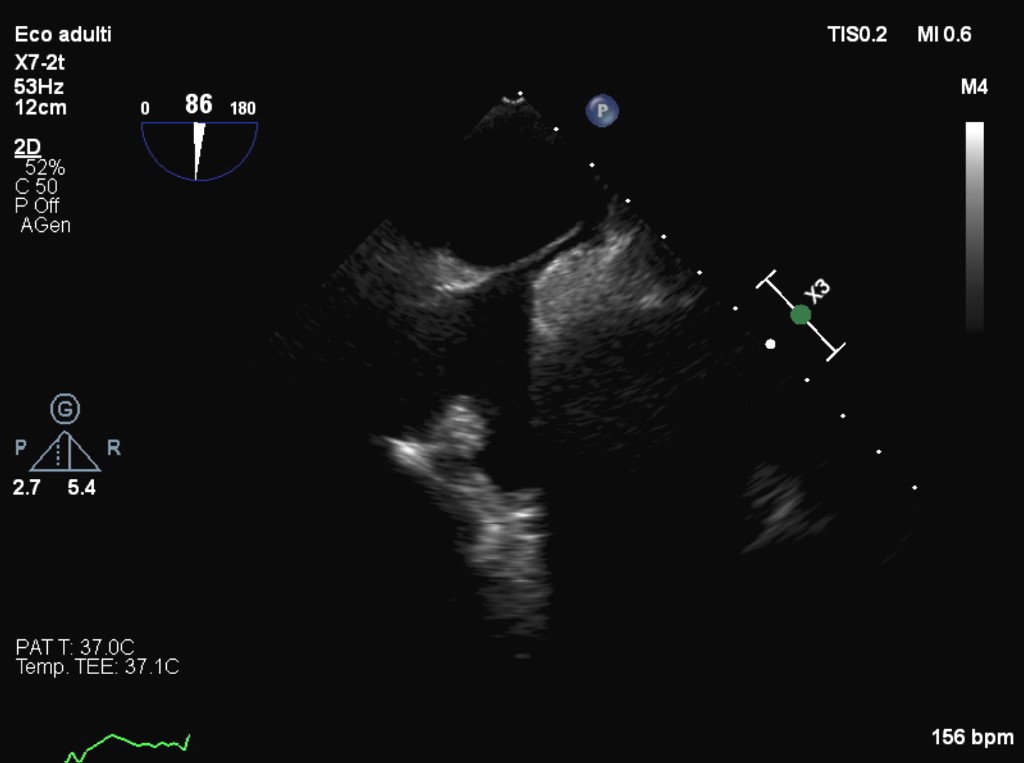
A 50-year-old man with obesity, dyslipidemia, and a history of renal calculosis presented to the Cardiology department with an infero-lateral ST-segment elevation myocardial infarction. Emergent coronary angiography revealed a circumflex artery characterized by multiple distal branch occlusions suspected for thromboembolism (file 2), with intravascular ultrasound showing partial recanalization of terminal vessels. Echocardiography demonstrated a left ventricular ejection fraction of 50% with basal inferior wall hypokinesia and mild aortic root ectasia. Given the angiographic suspicion of systemic thromboembolism of unknown source, an extensive diagnostic work-up was undertaken. Thrombophilia screening was unremarkable. No episodes of atrial fibrillation were detected during continuous monitoring. Transcranial Doppler identified a significant right-to-left shunt, confirmed by transesophageal echocardiography through a patent foramen ovale (file 1). Thoraco-abdominal CT did not show any thrombotic source. However, it revealed a non-calcific pulmonary nodule requiring surveillance, and at least five pancreatic lesions up to 2 cm with arterial-phase enhancement suggestive of neuroendocrine tumors. Laboratory tests showed persistent hypercalcemia and elevated parathormone consistent with primary hyperparathyroidism, while neuroendocrine markers remained within normal limits. Paratiroidectomy has been advised. The coexistence of pancreatic NETs and hyperparathyroidism raised a strong suspicion for multiple endocrine neoplasia type 1. Although no direct association between acute coronary syndromes and MEN syndromes has been reported in the licterature, MEN-related neoplastic disease may increase the overall embolic risk. Hypercoagulability is a clinically relevant concern in MEN1. Recent studies have demonstrated that patients with MEN1 have an increased risk of venous thromboembolism, with incidence rates two-fold higher than the general population. In the absence of a definite embolic source, it cannot be excluded that the increased thromboembolic risk and the anatomical predisposition associated with a patent foramen ovale may have contributed to coronary embolization. The patient was referred for multidisciplinary management. The patient remained asymptomatic on dual antiplatelet therapy. Genetic testing for MEN is ongoing. Patent foramen ovale closure was successfully performed.