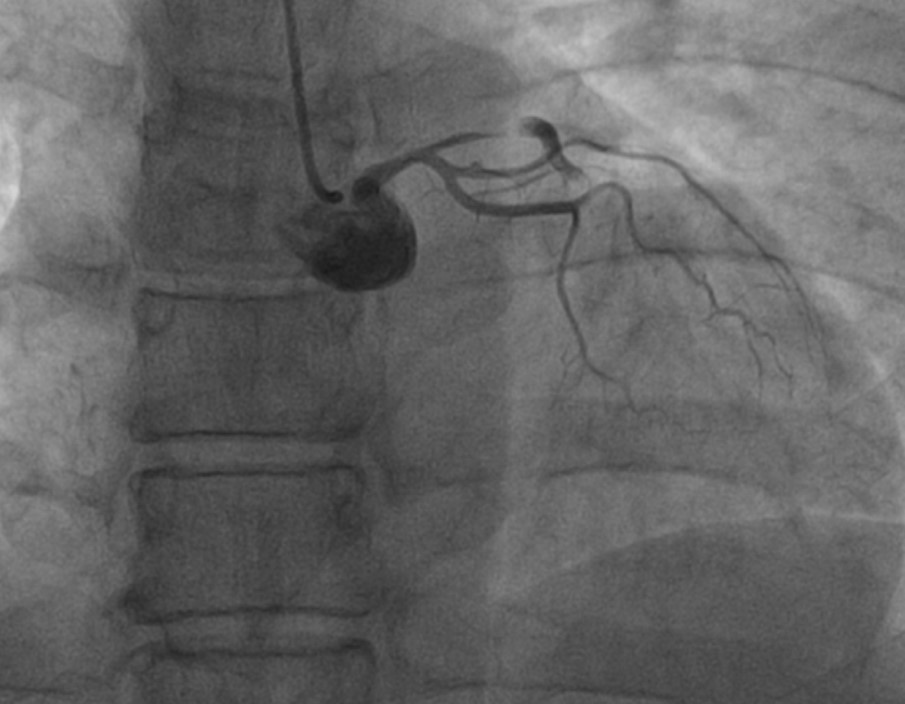
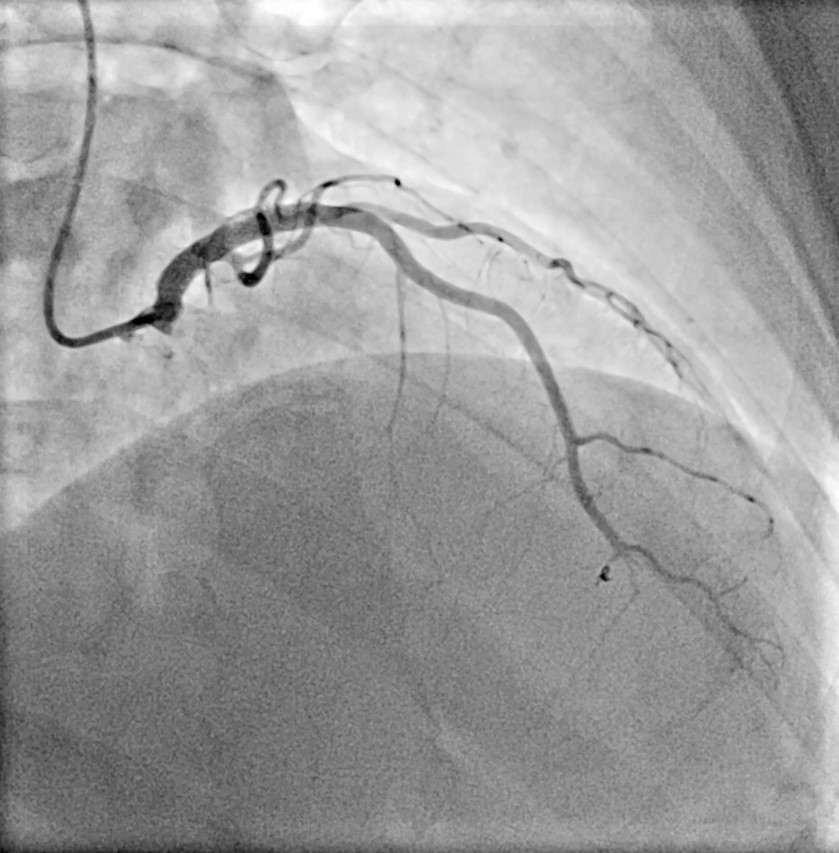
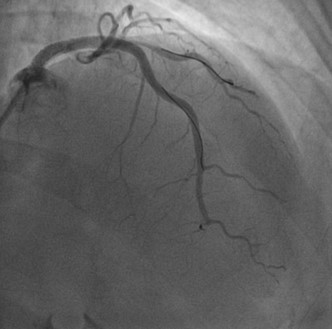
A 42-year-old female arrived to our hospital for epigastric pain: electrocardiogram (EKG) was negative and echocardiography normal but troponin levels were elevated. Coronary angiography revealed a spontaneous dissection of distal left anterior descending artery (LAD) – Type 2b according to Yip-Saw Classification1,2. No angioplasty was performed and she was discharged on Aspirin. Two days after, she was readmitted for a large anterior STEMI, first point of high-sensitivity troponin I (hs-TnI) was 5000 ng/L, prompting urgent coronary angiography which showed occlusion of the ostial LAD and wall hematoma, extending proximally to the left main (Figure 1). Pre-dilation of LAD was performed, resulting in occlusion of the the vessel and the diagonal branch, thus precipitating cardiogenic shock, needing noradrenaline. Stenting of LAD and left main was then achieved; diagonal branch remained occluded, with evidence of Circumflex coronary (CX) thrombosis and upstream of the stent in the left main (LM) (Figure 2). Due to persistent cardiogenic shock, a IABP was inserted. Intravascular ultrasound revealed stent malapposition, necessitating post-dilation in the diagonal branch. A iatrogenic small perforation in a distal septal branch required a microcoil insertion (Figure 2). Post-PCI echo showed akinesia of the apex and anterior wall with a reduced left ventricular ejection fraction (35%). The patient was transferred in ICCU, with weaning from vasopressors and IABP in one day. A cerebral magnetic resonance to exclude fubromuscular dysplasia was negative. A pre-discharge coronary angiography showed residual occlusion of distal LAD and complete recanalization of Cx (Figure 3; in few days ventricular function was full recovered. The patient was successfully discharged after ten days in good clinical condition with the following home therapy: cardioaspirin, clopidogrel, bisoprololo, pantoprazole, atorvastatin/ezetimibe2.