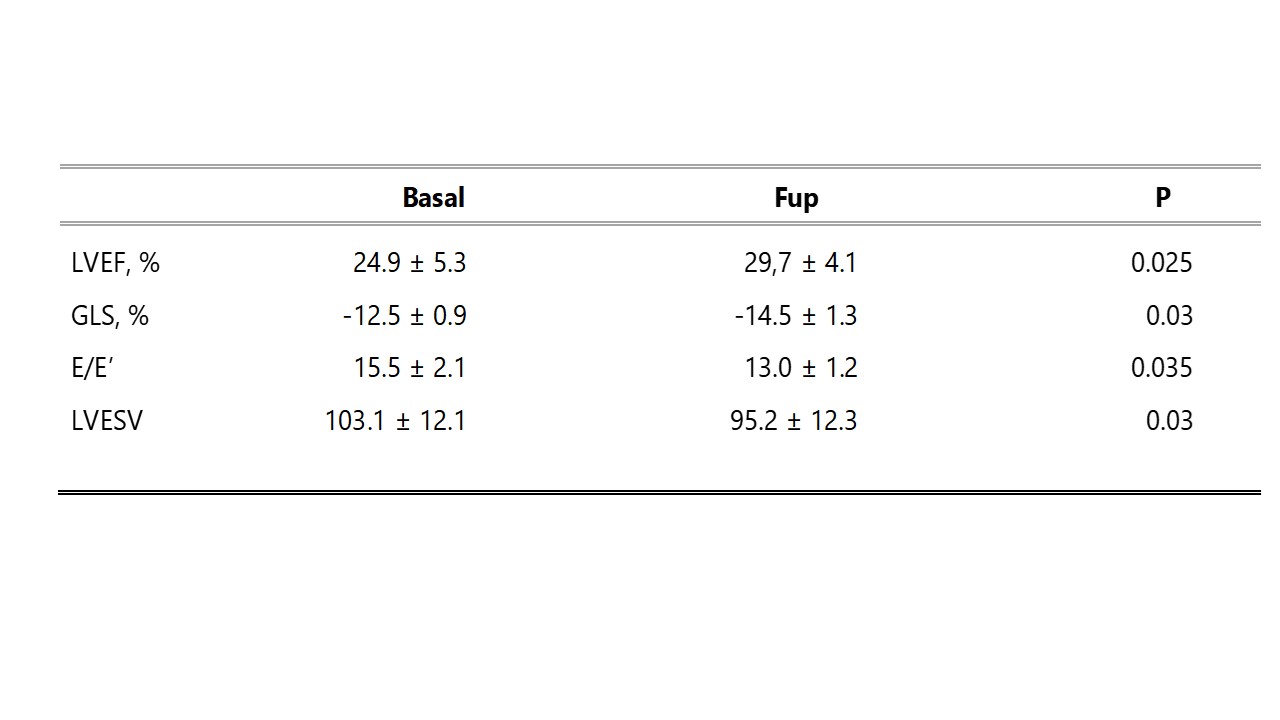
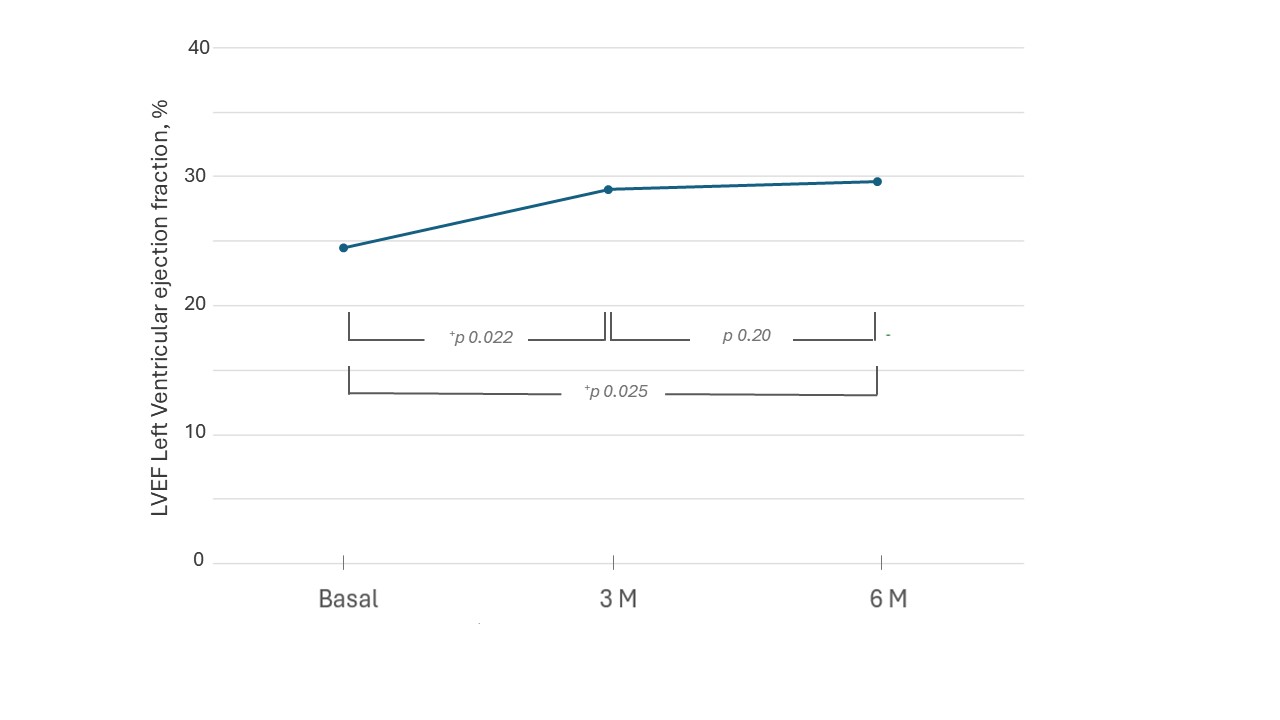
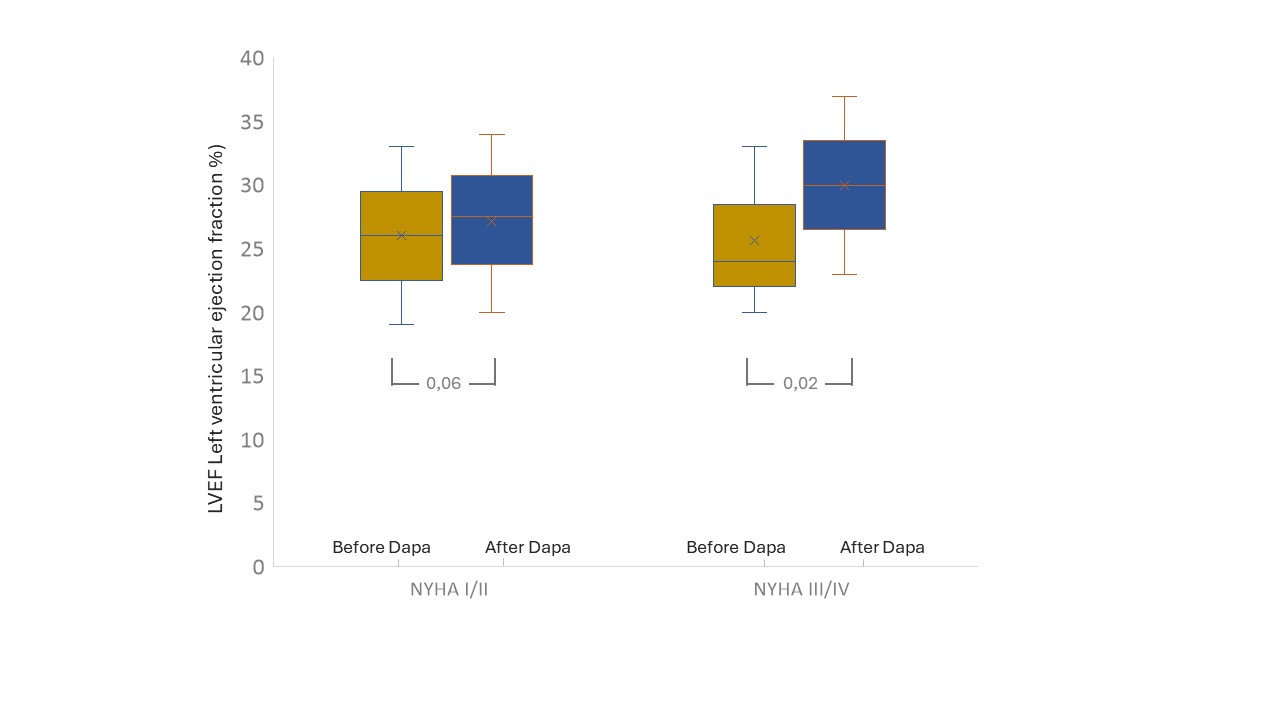
Aims: Dapagliflozin, a sodium-glucose cotransporter-2inhibitor (SGLT2) is approved for the treatment of heart failure (HF) regardless of ejection fraction. The aim of our study is to evaluate the effects of dapagliflozin in the medium and short-term on left ventricular reverse remodeling, correlating the possible improvement with the basal functional capacity. Methods: 87 outpatients (mean age 70.1±11.1years) with a known diagnosis of HF have been evaluated within a dedicated follow-up pathway according to a prospective observational protocol. Patients with HF with reduced ejection fraction (HFrEF) who had their therapy optimised with the introduction of dapagliflozin were observed. Echocardiographic parameters were identified at the time of introduction of dapagliflozin and during the observation period (3 and 6 months), evaluating the trend and correlating the changes with basal functional capacity. Results: Analysis of population data shows a significant improvement in the observation period (before vs after treatment) in mean left ventricular ejection fraction (LVEF) 24.9 ± 5.9% vs 29.7 ± 4.1% p=0.025, mean global longitudinal strain -12.5 ± 0.9 % vs -14.5 ± 1.3 % p=0.03, mean left ventricular end-systolic volume (LVESV) 95.2 ± 12.3 ml vs 103.1 ± 12.1 ml p=0.03, mean E/E’ 13.0 ± 1.2 vs 15.5 ± 2.1 p=0.035 (Tab 1). 52 patients (60%) had significant indices of reverse remodeling, identified in an improvement of LVEF >15%. Observing the trend of change in mean LVEF, there is a significant improvement at the 3-month control, and a subsequent plateau (Fig 1). Dividing the population according to basal functional capacity, it is observed a significant improvement of mean LVEF only in the group with the most impaired functional class. Mean LVEF in NYHA I/II group before treatment 26.7 ± 3.9% vs after treatment 27.5 ± 4.1 % p=0.06, mean LVEF in NYHA III/IV group before treatment 24.8 ± 4.1 % vs after treatment 30.1 ± 4.3% p=0.02 (Fig 2). Conclusions: In patients with HFrEF, dapagliflozin treatment produces an improvement of left ventricular systolic function in the medium-short term. This improvement is more evident in the first three months after treatment start and in patients who have a basal worse functional class. Therefore, we can hypothesize that hemodynamic improvement induced by treatment it contributes, at least in the medium to short term, to the improvement of structural remodeling.